

What Would Walt Disney Do? Part I—The Fragmentiest Place On Earth (TM)
(An Encounter in Three Parts)
by David E. McCarty MD FAASM (…but you can call me Dave)
26 October 2025
~ ~ ~ ~ ~
“We cannot solve our problems with the same thinking that created them.”
— widely attributed to Albert Einstein
~ ~ ~ ~ ~
PROLOGUE
In May 2021, I did something unthinkable.
I quit my job.
After a six-year tenure as Medical Director and full-time patient-centered clinician for the ambitious Colorado Sleep Institute project, I decided to hang up my spurs and ride off into the sunset. I was done.
I was done trying to communicate the vast complexity of Sleep Apnea to patients, one soul at a time. I was done trying to capture every nuance of that complexity in every single chart note, trying to prepare each and every patient for a journey across a fragmented healthcare landscape, a landscape in which their narrative would be replaced by a diagnostic label. I was done fielding red-hot complaints from other providers’ patients, always about the same issues, always about feeling disempowered in a vast and indifferent system.
Life-Fans, my beef was this: once you’ve seen what happens when your patients are empowered with the knowledge to make their own decisions, you never want to go back! This was my burden. This was my THING THAT CAN’T BE UNSEEN.
In May 2021, I quit my job, though it was untruthful--what I said before about riding off into the sunset. Riding off into the sunset was never my goal.
My goal was to teach what I’d learnt about patient empowerment to a larger audience. I was done doing it one person at a time. I wanted to teach the world…
My first attempts at a standard “book” were horrid. Frenzied, I’d write for 6-7 hours per day—planning indexes and chapters and table content--and then feverishly launching into it, day after day. For about five weeks, this was my pattern--manic attempts to capture that clinical wisdom before I lost connection with it forever--collapsing with a headache at the end of each day--sleeping with dreams of crawling things--awakening bleary-eyed in the morning to realize that what I’d written the previous day was utterly unreadable.
The harder I tried, the worse it came out. It was positively maddening. A psychological Chinese finger-trap.
What happened next was admittedly equal parts dismay and inspiration, a granny shot from half-court as the buzzer sounds, a delibulous yawp from a cornered animal with nothing to lose.
“Perhaps you’re going about this all wrong!” my brain snickered at me one morning. “You could reliably engage this information with your patients, person-to-person! Maybe it had something to do with…the conversation…maybe you need to explore this as a conversational exercise!”
The solution to this problem needed a different frame of mind. Einstein said so.
Something had to change.
I decided I needed a partner.
~ ~ ~ ~ ~
Enter Ellen Stothard, PhD
The first time I met Ellen was in 2017, when she presented her data from “The Camping Study” to our clinical group at CSI during one of our all-hands-on-deck conferences. To say I was impressed with her work is a massive understatment. I was blown away. I couldn’t believe what I was seeing. Right here in Boulder was an academic group that showed a virtual normalization of “social jet lag” and improvement in nocturnal sleep parameters after a 3-day camping intervention! They showed the world that Nature Therapy is real!
They demonstrated the medicinal effects of a campfire and a starry night!
And they were all over the science news for it!
Whaaaaaa?!! SO COOL!!!
Not long after that (perhaps in some small part, due to my unbridled and vocal enthusiasm for her work) Ellen was hired as CSI’s research and development director. With her guidance, CSI was able to put its research where its mouth was, demonstrating enhanced adherence and better outcomes using a fully integrated model—which is to say: a model where the clinicians were teamed with the equipment side of things to work together towards shared goals.
I’ll say this part plainly, so nobody has to decode it: it was Ellen’s knack for finding the story inside the data that allowed us to show the world that CSI patients did better when they didn’t have to leave…when they didn’t have to go “off campus” to another team to get their stuff! We finally had the data to make the claim that our patients did better with a unified team…when the clinical team shared a chart with the CPAP team…when we could talk to each other. It’s not rocket science, folks, but there you have it! Our group had the audacity to scientifically demonstrate it, and Ellen was in the cockpit.
At the time I cold-called Ellen in Summer 2021, I didn’t know her well. For example: I wouldn’t find out until much, much later just how hilarious she can be, when so inclined! What I did know was that she was sharp as a crease in a linen suit on Christmas, and that she was about as nerdy about SLEEP as anybody I’d ever met.
I had a strong hunch she’d be a good partner for a conversational deep-dive.
So, like I said, in June of 2021, I took a risk and cold-called Dr. Ellen Stothard, asking her if she’d like to do a PODCAST with me, called “Empowered Sleep Apnea.”
And, NO, I’ve never done anything like this before…
…and, NO, I didn’t have anyone else to help me…
…and, NO, I couldn’t pay her anything...
Y’all can understand why I gush with gratitude when I remember…
She said YES!
Cue angel choir singers as clouds part and brilliant sunshine fills the room…

Just a couple of SLEEP GEEKS, asking a few questions…
~ ~ ~ ~ ~
Summer 2021: we started recording. I’d decided that I would draw cartoons to go along with each episode, as an enticement to engage with the content. You know--BAIT, to drive visitors to the website, which was all part of my plan to teach the world all I’d learnt…blah…blah…blah.
Since that doorway opened, I’ve created hundreds of discrete cartoons for this project—doodles, one-liners, multi-panelers--many of which ended up in the “Beautiful Blue Book”, some of which turned into the children’s book The Nose Rules, others published in print circulation media platforms, like Dental Sleep Practice and SLEEP REVIEW.
Here’s something I’ve learned on this journey: There are cartoons that you draw because you’re trying to make a point…there are others that you draw because they make you giggle…and then there are cartoons that you draw because you can’t get them out of your head, and you are trying to figure out what they mean.
All of this hog-shazzle is to introduce the notion that this essay is about a cartoon that belongs in the third category, a cartoon that’s been bugging me ever since I agreed to participate in the Rebis Health project, a cartoon that takes on possibly the biggest existential crisis we face as an industry, and one which—I believe—has the power to lead us to our salvation.
But I’m getting ahead of myself, as usual.
My point here is that this essay series is the story of a cartoon, and—even better—what that cartoon showed me after it was drawn.
And to tell you this story, I feel like I have to start at the beginning.
The cartooning. That’s it.
I think the story has to start with the cartooning.
Cue spiral visual as we fade to an impossibly vividly remembered past…
voop! voop! voop! voop!
~ ~ ~ ~ ~
The Sketchpad Lens
All through my life, when the world stopped making sense, I drew it.
While other people kept journals or spreadsheets, I sketched absurd little universes. I’d draw pictures of my teachers. My friends. Anything that grabbed my interest. Cartooning wasn’t decoration so much as diagnostics on where my head was. Each frame was like a snapshot of my own cognition. I left graffiti everywhere.
Doodling became my lens. My homework in grade school would go forth, covered in cartoons. My class notes would sometimes get confiscated, torn up as idleness. In junior high, a kid publicly criticized my work in front of my friends—after that, I started hiding my habit from others. From then on, the cartoons were just for me—a way to personalize birthday cards and handwritten letters. A way to say DAVE WAS HERE.
I first went public with my cartooning habit during my two years at Cal State Fullerton, studying the sciences that my resume required to allow application to medical school. Another transition point in my life. Another time, when the world didn’t quite make sense. More on that in a minute.
In 2021, when Ellen and I began confronting the many challenges of how to address complex issues attached to Sleep Medicine, I found that my cartoonist’s pen could slip sideways through the tangle and come out the other side with a picture that said, “See? That’s the shape of it.” My old habit gave me what a standard hidebound textbook could not: Einstein’s change in mindset, the only solvent strong enough to dissolve a problem created by the old one.
That’s how I began to suspect that healing itself might be an act of re-seeing.
So, for the benefit of the reader, and to really add some fun stuff to this series, I thought I’d take this travelogue all the way back…to my cartooning bad-boy days…when the very strip I drew seemed delighted in emphasizing the darkness…
…cue theremin sound effects with a shimmering visual transition as we travel backwards in time…back to 1991…
~ ~ ~ ~ ~
DARKPlaces
Long before Empowered Sleep Apnea, long before Rebis, long before I had letters after my name, back when I was claiming my post-baccalaureate (go English majors!) science pre-med requirements at Cal State Fullerton, I drew a daily cartoon strip for the school paper, the Daily Titan.
The strip was called DARKPlaces
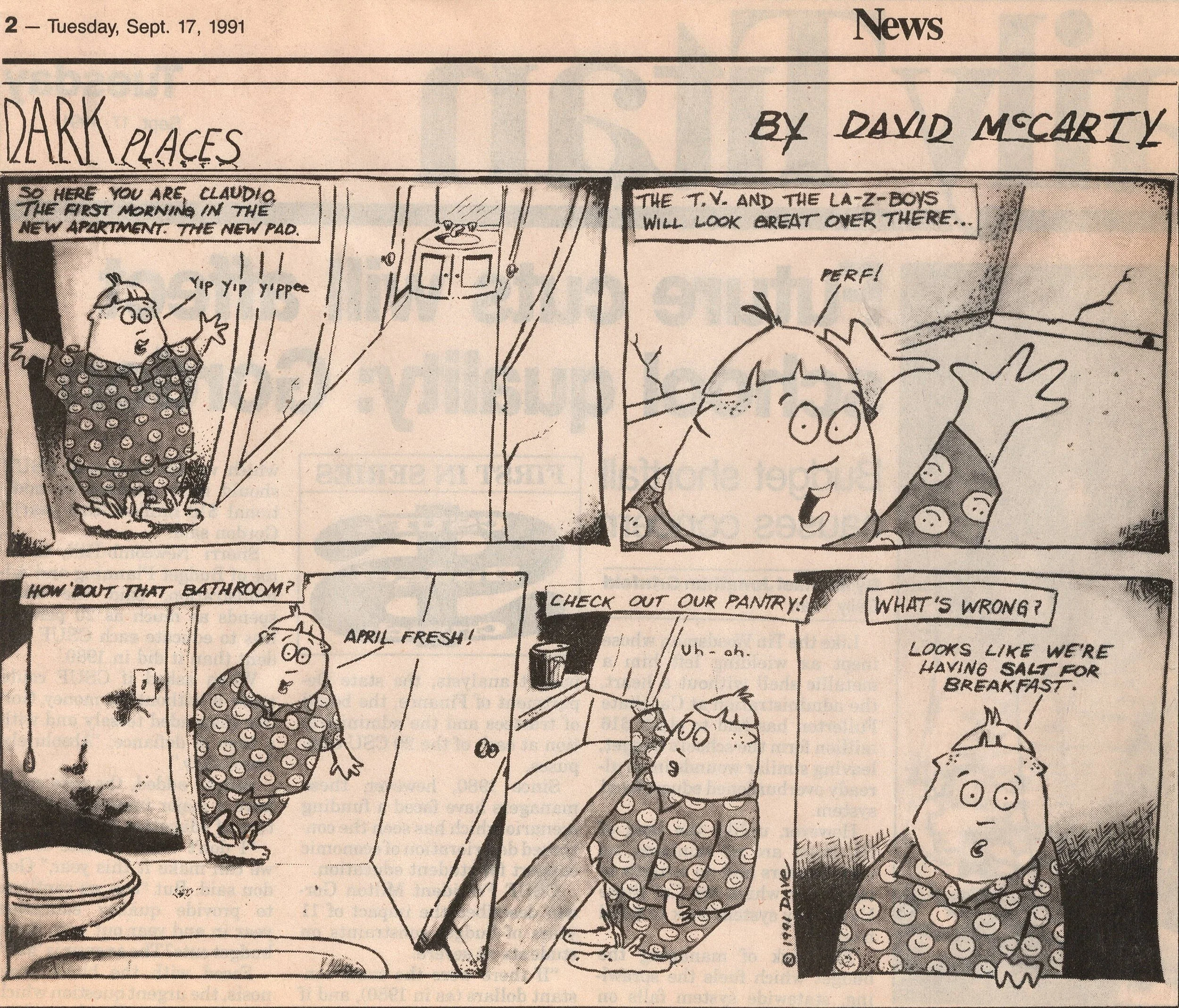
DarkPlaces DEBUT—Claudio Mahoney’s first appearance in print…on my 23rd birthday! :)
In it, a young man called Claudio Mahoney tried to find his way through a universe that Kafka would have found familiar, with barriers and non-sequiturs and hilarity all around, in family-sized servings. Indeed, this is how the universe looked to me, as I was busy readying to apply to medical school…seeing traps and barriers and added fees…starting to wonder if it was all some sort of cosmic joke?

Life Amongst the Litter: One-Way…DO NOT ENTER…No U-TURN…HA HA!
Years later, I realized that “ONE WAY” was the first map of a landscape I would spend decades exploring: a system so maze-like it could make even its initiates feel lost.
The Road to Nowhere that Talking Heads famously sang about was chillingly real. Turns out, I was just sketching the on-ramp.
Once inside the profession, I became an accidental anthropologist of the absurd. Medicine didn’t resemble a cathedral as much as an ant farm—clear walls, frantic traffic, no common song. Each discipline spoke its own dialect of certainty, its own little Latin. When data didn’t align, we threw rocks.
When the Empowered Sleep Apnea project started, I started drawing again, and, as I’ve mentioned, there were some images that wouldn’t go away.
The Winter of 2022 brought me one of those…one of those images that was trying to teach me something…an image I couldn’t get out of my head.
Silos. Dark, frowning, brooding. I saw tiny clinicians shouting at themselves, inside impenetrable fortressess of thought: “ENT!” “AADSM Dentist!” “AASM Sleep Lab!” “Airway Focused Dentist!”
A desolate landscape with a zigzagging pathway beneath…no one hearing anyone else…as a teacher, it was terrifying…and I was flummoxed!
How can I teach people who can’t even hear what I’m saying?
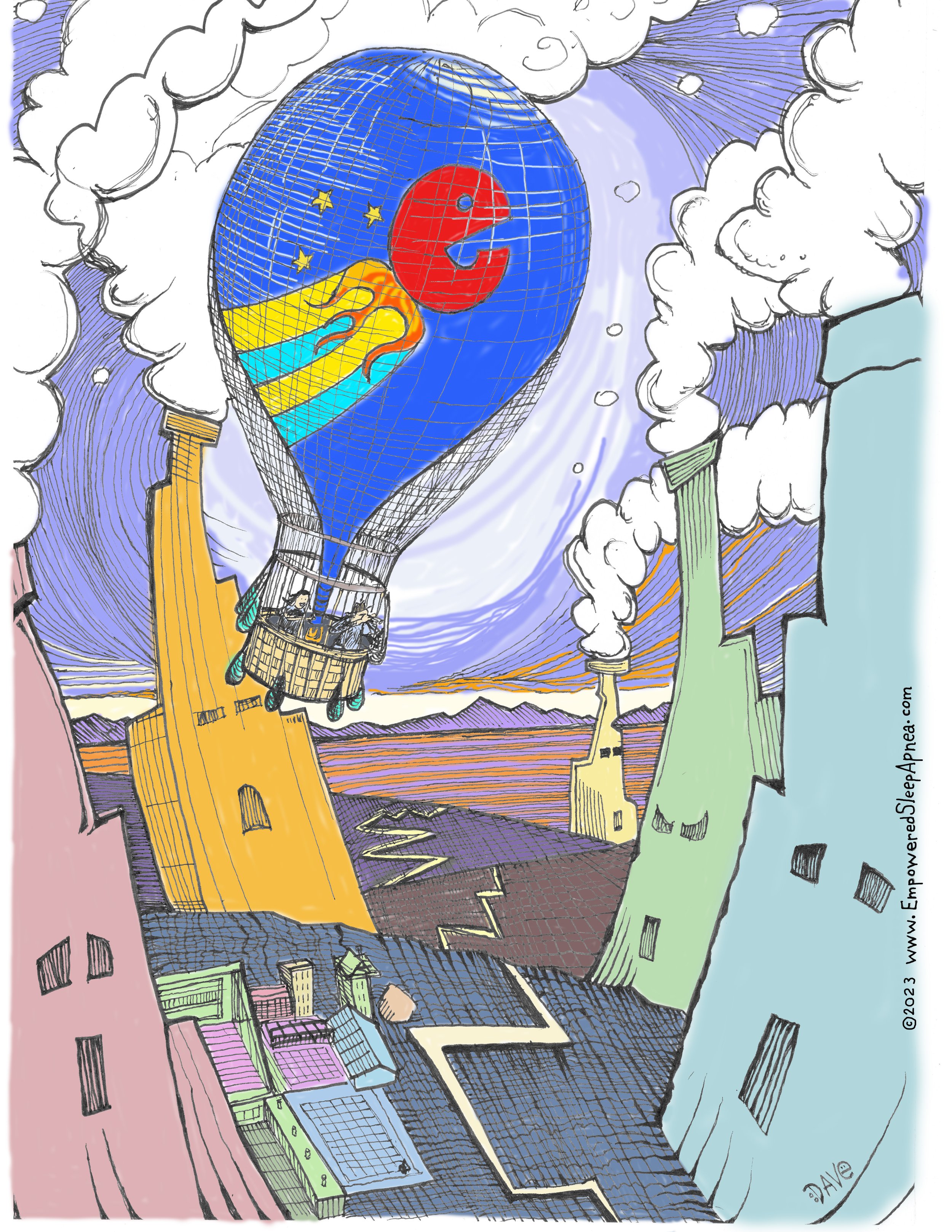
The cartoon—entitled “Balloon of a Different Color”—got me thinking about the whole subject of silos. It made it real to me. The realization of YES, THIS IS THE PROBLEM.
So, if siloed thinking is the problem, perhaps the first step in the process is understanding how silos work…why silos become the way they are…and why they stay that way…
It was around that time that I ran across the story of Ignaz Semmelweis—you remember?—the obstetrician who tried to tell his colleagues that washing hands could save mothers from horrible deaths due to childbed fever...
The world called him crazy. He thew invective rocks at his contemporaries until they institutionalized him, killed him, destroyed him.
You can look it up, what the world did to our hero, the Hungarian “Savior of Mothers.”
The world literally stomped him to death.
When I read that, I set down the book with a wordless “O” on my mouth. Never has the truth been more clear, and more chilling.
It doesn’t matter if you’re RIGHT! You could be right, and THEY can still snuff you out!
Psychologists call this tendency to stomp out what’s new The Semmelweis Effect.
All of this, somehow, seemed important.
~ ~ ~ ~ ~
I ended up telling Semmelweis’ story in the first episode to our PODCAST’s second season, PROLOGUE, the episode that became a keynote speech for Collaboration Cures 2023, a talk entitled The Silos of Sleep Medicine, The Semmelweis Effect, and the Blue Balloon Solution.
Here’s my point--the point is this: the cartoon led the way.
~ ~ ~ ~ ~
Since I published that cartoon, the Blue Balloon doodle has become a symbol for our collective flight of discovery. The Blue Balloon meant perspective—lifting above the silos long enough to see their pattern.
Since its inception 9/6/22, the Empowered Sleep Apnea project has grown into a fully RAD PODCAST with two seasons of original material, two books, this blog, a few scattered op-eds in other settings, multiple talks and webinars, numerous cartoons appearing in circulation media, and a fellowship of clinicians and patients asking better questions.
Funny thing: since I agreed to participate in the Rebis Health clinical project—which is to say since January of this year--my frame of reference has been a bit different. From my new perspective, I see a landscape that’s much more dynamic and colorful than my prior iteration of dark frowning silos and zigzag paths.
Launched from Rebis’ shores, our Blue Balloon has taken us to terrain that smells like popcorn and broken dreams, and the carnival music is sometimes drowned out by crying.
I finally drew it. The cartoon that’s been nagging my head for months.
It’s time we talked about it...
~ ~ ~ ~ ~
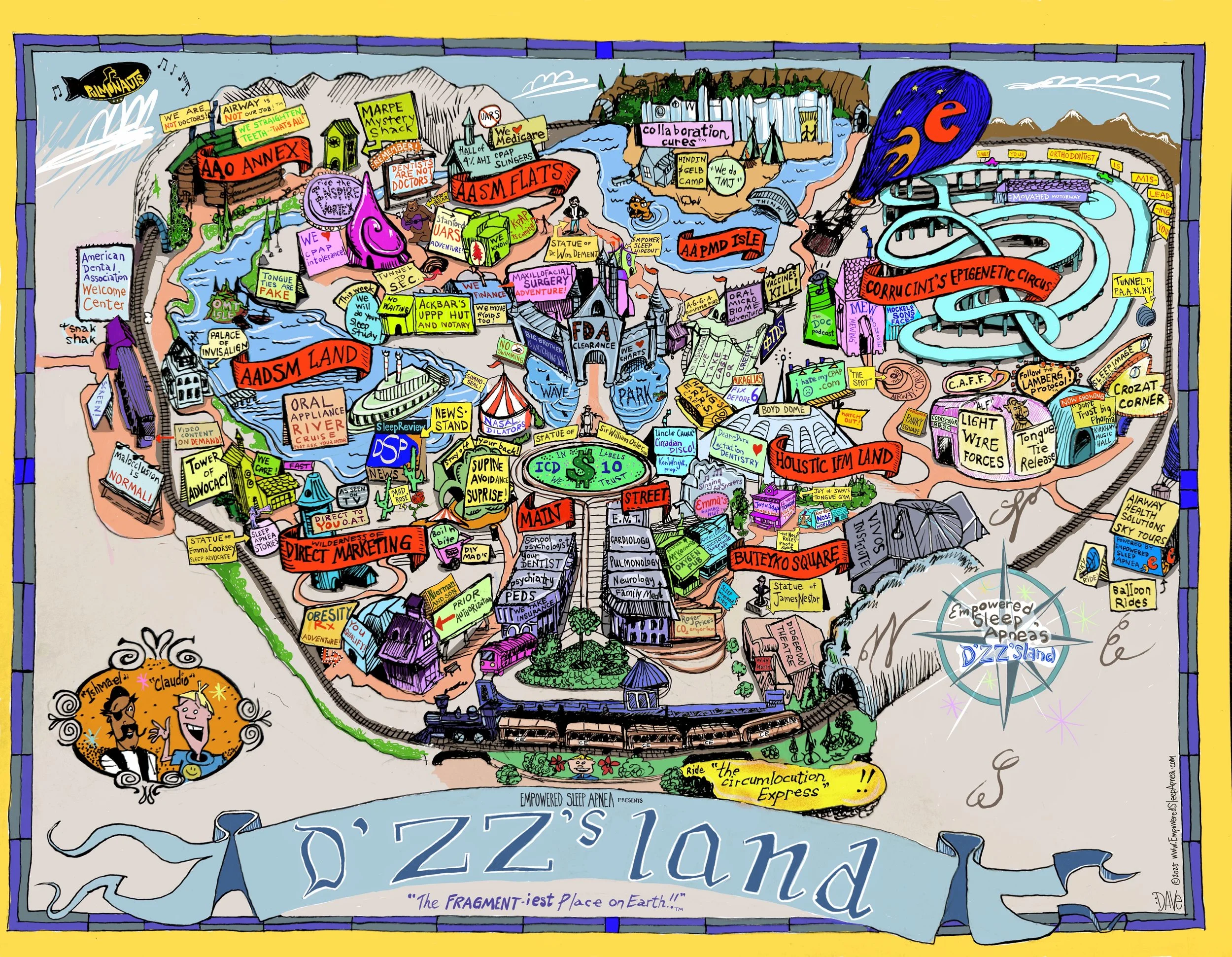
The Fragmentiest Place on Earth TM
The music is deafening, the smell of popcorn makes you swoon, and the view is startling.
Each specialty is its own attraction: visit the 4% AHI CPAP Slingers!...tour the Direct Marketing Wilderness…sojourn at AAPMD Isle!
When we walk along the causeway, we see lost souls, drifting aimlessly…the maps blowing about on the constant wind contradict each other…tickets for the attractions aren’t always covered by insurance…guests wander about, clutching referral forms like broken fast-passes.
Everyone swears they know where they’re going, but nobody agrees where it is!…worse!...few people can tell you why they’re even there!
Welcome to the park we all play in.
Welcome to The Fragmentiest Place on Earth ™.
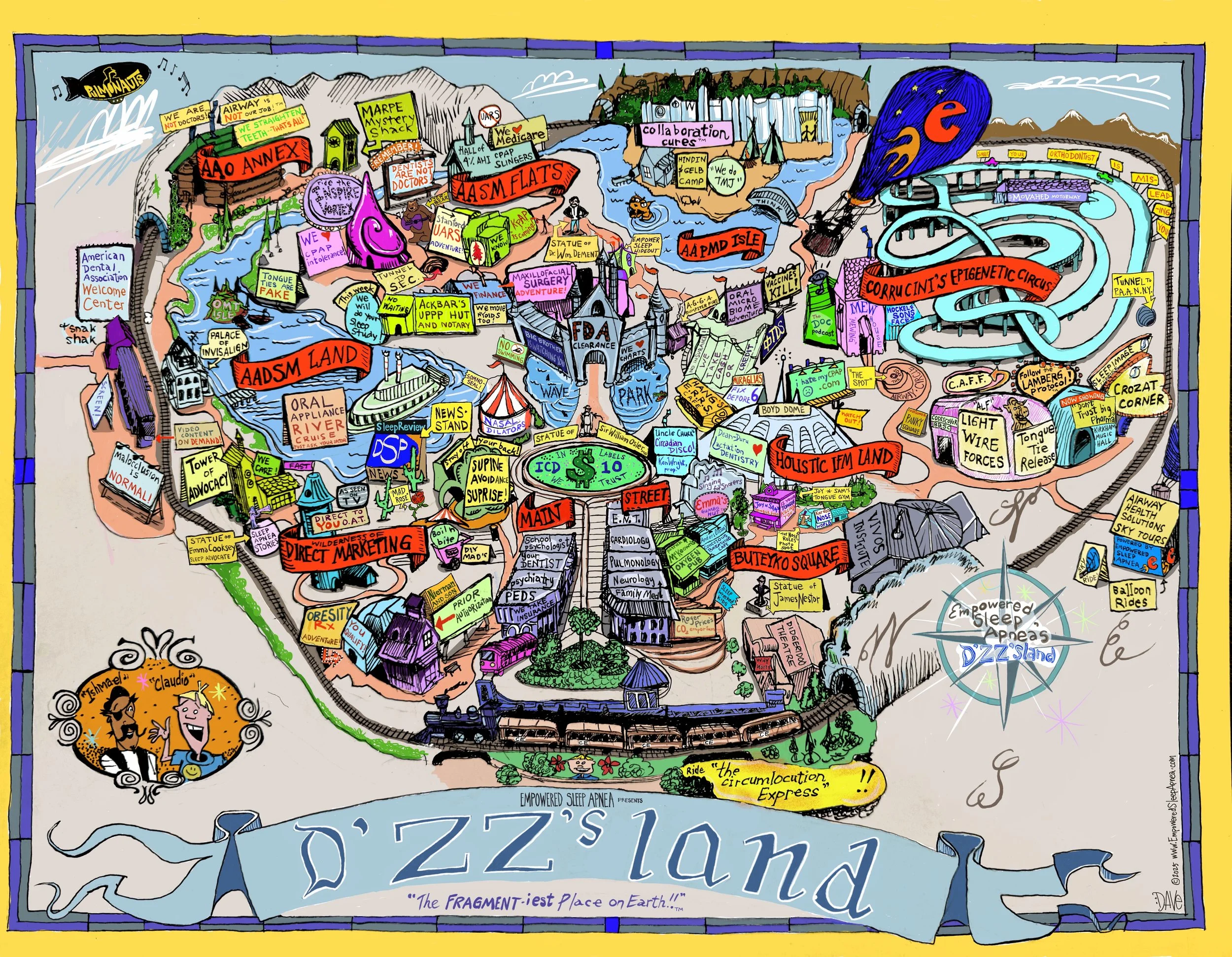
Empowered Sleep Apnea presents: D’Zz’s Land—THE FRAGMENTIEST PLACE ON EARTH!!
The cartoon practically drew itself—I pictured Claudio at the gate, hopeful, ticket in hand, staring into a kaleidoscope of chaos, a riot of colors, heaps of patient-facing propaganda and lots and lots of white coats.
Somewhere inside that mess, I sensed a story trying to teach me something: that the frustrations our patients face aren’t technically individual treatment failures; that somehow, it’s larger than that.
It’s a park-wide problem.
It’s the recognition that when coherence breaks, suffering multiplies, and no one quite has the language to talk about it. When I’m talking about coherence, here’s what I mean: I’m talking about agreement on fundamental language pertinent to three questions.
Three Fundamental Questions. Three Foundational Questions.
Three Questions that link us all together…
I got to thinking it’s time we all figured out what we’re going to say.
Here’s the problem: if you go to different attractions in our fictitious amusement park, you’re bound to get very different answers to our three foundational questions. And, if we trace that drama out, we start to glimpse a strange new flavor of suffering that’s introduced into the whole experience…an existential suffering that’s hard to describe…when our day-to-day life is all about how things are going, in our part of the park, for the ones who happen to stay on our ride, it's hard for us to see...
It’s the suffering of finding oneself out on the causeway…in between the rides…not knowing who to trust…
SO: What are these three questions, then, the questions that lead to so much confusion?
Read on, dear explorer, read on…
~ ~ ~ ~ ~
Three Questions to UNITE Us All

Now we finally know what those three stars are for! :)
The reader will note that within the official Empowered Sleep Apnea logo is a blazing letter “e”—we call him “happy e”—who is perpetually rocketing skyward on flames of curiosity and self-fulfillment. Blazing in the field behind him are three five-point stars …I drew them, I should know. I always thought they were just decorative. Now I know better.
Their meaning has finally been revealed to me:
Life-Fans, we have not one North Star, but THREE.
Life-Fans, these stars represent the three questions that can unify our park. A different kind of Pyramid-Scheme (lol), ours is a constellation of STABILITY, a Constellation of Empowerment.
Three stars… Three Questions:
What is Sleep Apnea?
Why should we treat it?
What else could this be?
As I surveyed the rides and attractions in our park, I could see that these questions are answered differently…depending on where you land in the park…depending on which ride you choose to take. Sometimes, the answers to these questions make people fight with each other. Sometimes, the differing responses make patients lose all hope, seeing no trustworthy path forward.
And over all of it floats the Blue Balloon.
So…let us drift toward the gates of that broken amusement park and see if we can recognize our story within it. Inside waits a tour we must take together—a chance to see how every ride, every vendor, every earnest operator answers those same three questions in a different dialect.
So…dampen the flames for our hot air balloon as we descend…disembark… grab a frozen banana, and remember…as we tour…keep your hands and arms inside the vehicle at all times!
The show is about to begin.
~ ~ ~ ~ ~
What is Sleep Apnea?
Before going any further, let’s agree on some terms. When it comes to sense-making, the names we have for things—the very words we choose—the labels we assign--carry immense power. To hear complexity sensemaking expert Dave Snowden put it:
“Names of course play a major role in human sense-making and carry with them historical meaning and implications for action. Names carry with them power, as any reader of myths and legends will tell you.”
Snowden, D. (2011, October 22). Typology or taxonomy? The Cynefin Co. https://thecynefin.co/typology-or-taxonomy/
So: does this person “have” Sleep Apnea…or not? What about “upper airway resistance syndrome?” Which label should we use?
Depending on which part of the amusement park we decide to visit, we might get different answers! Perhaps even more frustrating, none of the ride operators seem ready to take responsibility for the comic degree of confusion taking place in real time. Perhaps even worse, nobody seems to notice there’s even a problem!
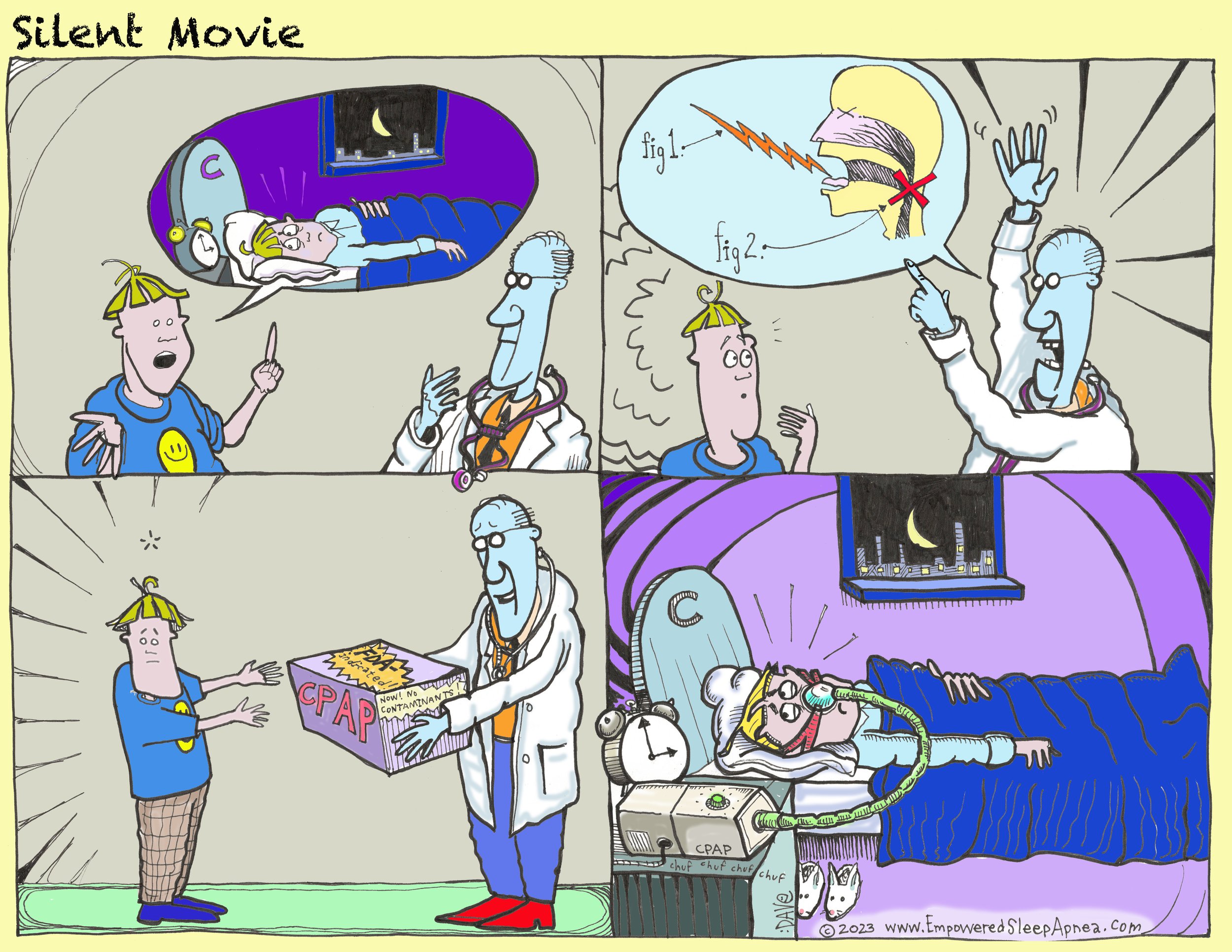
Here’s how this drama played out in one cartoon panel:

A simple question? Depends on which head is talking…
The truth is, it’s easier than ever to achieve the diagnostic criteria for Obstructive Sleep Apnea (ICD-10 G47.33). According to the most recent iteration of the International Classification of Sleep Disorders (ICSD-3-TR), all that’s required are “symptoms that affect sleep-wake quality of life” and 5 obstructive events per hour of sleep.
Here, “obstructive events” includes apneas, hypopneas, and respiratory effort related arousals (RERAs).
Whaaaaaa? True story! That’s it! 5 RERAs per hour + complaints = diagnostic. BOOM!
Get this, it gets better: If you have 15 obstructive events per hour, you fulfill diagnostic criteria, even with no symptoms at all. BOOM! BOOM!
This is where the fun begins, though.
See, scoring RERAs are not “required” for a lab to maintain AASM accreditation, so many labs simply opt out. Simpler. I’ve always found it a bit odd, and have wondered whether these labs shouldn’t come with a disclaimer? LOL!! Maybe something like…
Warning: our lab does not score RERAs and is therefore under-powered to reveal non-desaturating sleep-fragmenting events! Our lab should be considered to have a high false-negative rate. So…buyer beware!! If we tell you that you don’t have “Sleep Apnea” you should seek another opinion!
What about UARS? The term “upper airway resistance syndrome”—developed at Stanford as a way of talking about non-desaturating patients who benefitted from CPAP—has been officially retired by the AASM, but it continues to have relevance – and legs – in airway focused dentistry circles, precisely because of the scenario playing out as described above, where non-desaturating events are simply not acknowledged. In some circles, getting folks going about UARS can get tempers going, and might start a fight. I’m not joking. The language divergence was powerful enough to manifest the collaborative rock band PULMONAUTS, as the founder of the band, Dr. Tom Colquitt, could tell you himself. That’s powerful!

STANFORD: the mother ship of SLEEP!
It's fun to laugh, but what about an example from real life?
Patient synopsis: 52-year-old woman with Medicaid insurance. 6/10 sleep satisfaction due to frequent awakenings, occasional awakening with gasping, nocturnal wheezing, and daytime sleepiness (Epworth Sleepiness Scale score 12/24). Vulnerable comorbidities included migraines and a personal history of traumatic brain injury, with persistent daytime neurocognitive impairment symptoms.
In spring of 2025, the patient underwent an in-lab polysomnogram at an AASM-Accredited sleep center. The study demonstrated a CMS (4% desaturation criterion) AHI of 4.4/hr and an AASM (3% desaturation criterion) AHI of 9.4/hr. The lab had opted out of scoring Respiratory Effort Related Arousals (RERAs), so the respiratory disturbance index (RDI)—which tallies up all apneas, hypopneas and RERAs—was not reported.
If you’re doing the math, you can already see that, given the symptoms, the patient has met the ICSD-3 diagnostic criteria for obstructive sleep apnea (G47.33). The AASM AHI was 9.4…if RERA’s had been scored, the overall obstructive event rate likely would have been higher. As we noted, given her symptoms, she only needed an event rate higher than 5 to cinch the diagnosis…
So, given that we’ve established that “naming” is important when it comes to complexity sense-making, I’m starting this tour with an actual screen shot of how this “naming” exercise went down, this time, for this patient, under the care of this physician, who will mercifully remain unnamed.

Warning: this “actual” sleep study report contains “factual” problems!
Heyo! Whaaaaaaa? In this instance, in this part of the amusement park, the answer to the question “Do I have Sleep Apnea?” apparently depends on your insurance class and what that organization decides to pay for! Yikes!

The Three Questions: Hall of 4% AHI CPAP Slingers Edition!

This is where the park gets interesting, folks, so stay with me.
Let’s deus ex machina our patient out of the Hall of 4%AHI CPAP Slingers, and into an office prepared to discuss approaches like expansive orthodontia and oromyofunctional therapy…someplace over near Corrucini’s Epigenetic Circus and Buteyko Square…let’s have her see an Airway Focused Dentist!
We’ll see that the fun begins when the language starts to drift…

We note immediately that the vibe is different in this part of the park, the ride vendors aren’t trying to run us off! Far from it! In this part of the park, they seem to know all about how the AHI is used as a barrier for care. They understand that non-desaturating events are important!
Some of them have even gotten tired of pretending that they don’t know it! LOL!
We put our ear to the door and hear the conversation unfold…
• “With the AASM AHI of 9, You actually DO meet the criteria for the diagnosis of OSA—it’s just that treatment won’t be covered for you under Medicaid…”
• ”Oh, and by the way, it’s not sleep disordered breathing, it’s “breathing disordered sleep”…”
• “You’ll need two years of work-intensive orthodontia.”
• “Your sleep doctor doesn’t know what he’s doing.”
• “The AHI is a meaningless metric”
• “Your health insurance won’t pay for any of this.”
Try not to worry, Life-Fans, if you have a strange feeling in the pit of your collective stomach! That’s just the lack of cohesion talking again! Let’s run this ecosystem through the Three Questions and see what we get…
The Three Questions: Airway Focused Dentistry Edition!

This version deserves some comments. First of all: BRAVO! The language here is getting closer to something resembling the living breathing beast walking around with the name “Sleep Apnea”...
For the first question, we see a new narrative developing, one involving posture, form & function, one that’s taking us into a whole new understanding of developmental biology! This makes it exciting, and also very new to many people.
For the second question, we see dentists shouldering a new role that is now strangely seemingly somehow at odds with traditional medical care, making collaborative management even more challenging. How can one collaborate with someone that’s apparently part of the problem?
For the third, we see an explosion of interest in root cause discovery, with massively divergent habits in different practice cultures, depending on where you happen to be. Again: cool, but new!
And that’s important.
I’ll switch gears here and note that Carl Jung—the iconic psychiatrist who explored the notions of The Collective Unconscious and Synchronicity—believed that it was human nature to fear the unknown, the new, the next-level. Speaking of names (and their importance) he even gave this idea a name with a classic feel: misoneism--from the Greek misos (hatred) = neos (new).
I think that’s the best way to introduce what happens next in our triptych story.
See, the newness of it all is a character to be reckoned with, and the misoneism pays a visit.
One size fits all? Maybe somebody shoulda clarified his NARRATIVE! :)
~ ~ ~ ~ ~
“Ask Your Doctor”
The patient left the Airway Focused Dentist’s office with a yucky feeling in her stomach. It sounded legitimate, but that price tag! Maybe they were just trying to sell her an expensive therapy? And what’s all this talk about “Breathing Disordered Sleep”? Now that she’s had a moment to get her head together, it all sounds so fantastical! What’s a Self-Respecting Patient to do?
After some solid hand-wringing and a phone call to her best friend, she’s decided to check in with her primary care provider, a kind and cordial (but overworked) family practice Physician Assistant at a clinic that takes her insurance, which (these days) is hard to come by.
What’s the visit for? She had concerns, you know? About this different language the dentist was using…about what she should do next? Reason for the visit, the receptionist wants to know? Oh, she didn’t know…just put “fatigue”…

It takes two weeks to get an appointment. She has fifteen minutes to state her case and get out. Although the conversation is muffled, we can’t help but overhear some of the teaching points…
• ”Dentists are not Doctors”
• “The only treatment for Sleep Apnea is CPAP and a mandibular advancement device—those other options have no data and they are a scam”
• “Your primary sleep doctor said you don’t have Sleep Apnea, so you must not need CPAP…”
• “Maybe you need a referral to psychiatry?”
Here’s some follow up: the patient initiates medication for the treatment of insomnia and anxiety, and leaves a 1-star Google review for the Airway Focused Dentist.

The Three Questions: PCP Edition!

Once again, there’s that sense of vertigo, that lack of cohesion…
…for the first question, when we’re busy, we think of “Sleep Apnea” as being defined by the traditional treatments covered by insurance.
…for the second, we see the sad results of specialization—the specialists’ word is considered the final say on the matter, and the matter’s not up for debate!
…for the third question, we see the arbitrary nature of complexity management within medical diagnostics, on display, in full view. If it’s not Sleep Apnea, perhaps it’s…um… depression?…
Three different clinical settings…three different “rides” in our Fragmentiest Place on EarthTM…three different sets of responses to the THREE QUESTIONS that make our world go ‘round:
WHAT IS SLEEP APNEA?
WHY SHOULD WE TREAT IT?
WHAT ELSE COULD IT BE?
~ ~ ~ ~ ~
As the sun descends on D-Zz’s Land, the Main Street Electrical parade of biologic weight loss options begins, and skyrockets and fireworks will soon brilliantly illuminate the night sky. We decide to call it a day.
We limp back to the parking lot--tired, confused, nauseated, sunburnt and broke.
The car has been stripped and ticketed.
A note is under the windshield wiper.
It reads: We hope you enjoyed your visit! Come back real soon!
~ ~ ~ ~ ~
David E McCarty MD FAASM is the Chief Medical Officer at Rebis Health and the co-creator (with Ellen Stothard PhD) of the Empowered Sleep Apnea project. He will be back next week with Part 2 of this 3-part series: What Would Walt Disney Do? Part 2—The Happiest Place On EarthTM