

An Empowered Response to the AASM Guideline on Combination Therapy for Insomnia
OR: It’s Not a LABEL, it’s a PROCESS!
~ ~ ~ ~ ~
By David E. McCarty, MD, FAASM (…but you can call me Dave)
10 May 2026
~ ~ ~ ~ ~
“To study the phenomena of disease without books is to sail an uncharted sea, while to study books without patients is not to go to sea at all.”
William Osler, MD [1]
“A map is not the territory it represents.”
Alfred Korzybski [2]
~ ~ ~ ~ ~
An Engineer, a Broken World, and a Question about Language
In 1933, a Polish-American engineer and philosopher named Alfred Korzybski published a dense, eccentric, and strangely prophetic book called Science and Sanity.[2] At the time, the world was apparently unraveling: industrialization had accelerated faster than human wisdom, propaganda and ideology were replacing direct lived experience, and the global economy was a smoking hole.
Marinating in this hot geopolitical mess, Korzybski became fascinated by a deceptively simple question:
How do we humans become trapped by the words we use?
Words, a prison? Really?!
Korzybski thought so, observing how we routinely confuse our descriptions of things with the things themselves; we create labels, categories, and conceptual maps so we may navigate complexity, but then (perhaps proud of the language we’ve created), we come to forget that the map is only a representation. Eventually, the abstraction ossifies, and the word starts to feel more “real” than the underlying phenomenon it was meant to describe.
When I say Korzybski was fascinated with this idea, I’m not playing. It was more like an obsession. During his heyday, he made a thoughtful swing at re-inventing human scientific thought, creating a philosophical framework he called General Semantics, a discipline concerned with how language shapes perception, reasoning, and human behavior.[2]
Cover Art for Korzybski A. Science and Sanity: An Introduction to Non-Aristotelian Systems and General Semantics. 5th ed. Brooklyn, NY: Institute of General Semantics; 1994. [9]
Korzybski’s following was almost cult-like; Buckminster Fuller and Robert Heinlein were among his many fans. Though largely forgotten today outside specialized circles, his central warning from long ago now feels oddly modern. See, looking back at his work, it all feels eerily similar to one of the central tensions we’re now experiencing in the field of Sleep Medicine today. Now that it’s on my mind, it’s hard to let it go.
You might say the idea is…keeping me up at night, which is appropriate.
After all, the paper that I want to poke at is all about “insomnia.”
~ ~ ~ ~ ~
A New Guideline and a New Question
I’d call the recent American Academy of Sleep Medicine (AASM) Clinical Practice Guideline on Combination Therapy for Chronic Insomnia an ambitious and noteworthy document.[3] It’s careful, restrained, appropriately evidence-based, and transparently honest about the limitations of current knowledge. The recommendations are conditional, the certainty of evidence is low, and patient values and preferences are emphasized repeatedly throughout the text.[3] This is not the language of arrogance, folks; it’s the language of a field attempting to navigate genuinely complex territory, responsibly.
Nevertheless, I found myself thinking (as I’m wont to do) about language, about Korzybski’s obsession, and (subsequently) about what to make of all of this. I can’t shake the feeling that beneath this document’s thoughtful recommendations, there’s a deeper question, one that’s perhaps so pervasive that it simply goes unasked:
What prison do we enter when we use the word “insomnia”?
~ ~ ~ ~ ~
Word Nerds and the Foundation of Reason
This little diatribe may initially sound like some sort of semantic exercise (in the pejorative sense), as if discussing the meaning of words is the territory of nerdy eggheads.
That’s the point, I guess. Korzybski’s central insight with his project is that the things we say are never “just words.” Language (he argued) shapes the pathways through which inquiry unfolds. Once a phenomenon receives a “label”, the label itself begins influencing what questions are asked, which mechanisms are considered, and which treatments feel intuitively appropriate.
In medicine, most folks would agree that this process is unavoidable: diagnostic language is essential for communication, research, epidemiology, reimbursement, and clinical reasoning itself. Without the abstraction of discrete diagnoses, medicine would collapse under the sheer complexity of biological reality.
The teaching point? Korzybski’s General Semantics reminds us about the background risk of this process, about the inconvenient observation that it substantially changes human cognitive processing.
The risk is not that labels exist.
The risk is forgetting that they are labels.
~ ~ ~ ~ ~
Tension in Label-Land
The AASM guideline offers a revealing example of this tension. Chronic insomnia disorder is defined clinically through symptoms of difficulty initiating sleep, maintaining sleep, or waking earlier than desired, accompanied by distress or functional impairment.[2] No objective testing is required, meaning the diagnosis ultimately depends upon clinical interpretation of subjective experience.[2]
At the same time, the actual management of the thing we call “insomnia” unfolds across a remarkably broad physiological and psychological terrain. The guideline discusses sleep continuity, daytime functioning, fatigue, anxiety, depression, quality of life, medication effects, treatment adherence, patient preference, and differing therapeutic goals.[2] The clinician is reminded to individualize care continually, balancing competing priorities and adapting treatment to the lived experience of the patient.
In other words, though the guideline insists that “insomnia” is a diagnostic category, it simultaneously recommends managing it as a multidimensional process.
The unexplained tension of this duality reveals something important. Most clinicians recognize the “process” part of the insomnia experience intuitively. A patient who cannot fall asleep because of delayed circadian timing is not experiencing the same underlying process as a patient whose sleep fragmentation arises from untreated obstructive sleep apnea, chronic pain, hypervigilance, stimulant use, grief, trauma, or restless legs physiology. The word insomnia may apply to all of them (perhaps self-applied, perhaps “diagnosed” by someone in a white coat), but the mechanisms and potential solutions for each of these scenarios would be profoundly different.
Here’s the thing, Life-Fans: once the label enters the conversation, a subtle psychological shift occurs; the abstraction starts to feel sufficient, satisfactory, explanatory.
This was precisely the phenomenon Korzybski warned about nearly a century ago: the map masquerading as the territory itself.
~ ~ ~ ~ ~
Fighting Words
Here’s something to contemplate: “INSOMNIA” (as a word) makes people fight!
Why? Maybe it’s because it means different things to different people! One clinician may wax eloquently about behavioral conditioning, while another focuses on micronutrient repletion. A clinician caring for war-torn veterans may see it framed through the lens of psychiatric hyperarousal, while an airway focused dentist might spot upper airway resistance and the dysautonomia of elevated work of breathing hiding beneath all of it.
Meanwhile, every patient experiences something akin to “my sleep at night is broken.”
Look deeper, and we’ll see that what appears to be disagreement about treatment is (in reality) disagreement about the underlying process concealed beneath a shared label…beneath that trusty but troublesome word that makes people fight…beneath the “diagnosis” of “insomnia.”
This is why conversations about insomnia can become strangely circular. Folks use the same word while referring to entirely different physiological realities.
Korzybski’s lens gets useful here, reminding us that abstraction necessarily removes detail. Indeed, each successive layer of description simplifies reality further: the patient’s lived experience gets translated to named symptoms; symptoms collected together become syndromes; syndromes get reduced to diagnostic criteria, which ultimately crystallize as billing codes and treatment algorithms.
At every stage, complexity is reduced.
I’ll say it again, so it’s clear I’m not complaining: this reduction is necessary. Medicine could not function otherwise! However, when abstraction becomes too rigid, curiosity begins to narrow around the category itself rather than the processes producing it.
That’s where the trouble starts, you see? That’s the tipping point, when solutions become label-based, and the monster we’ve created walks and talks on its own.
~ ~ ~ ~ ~
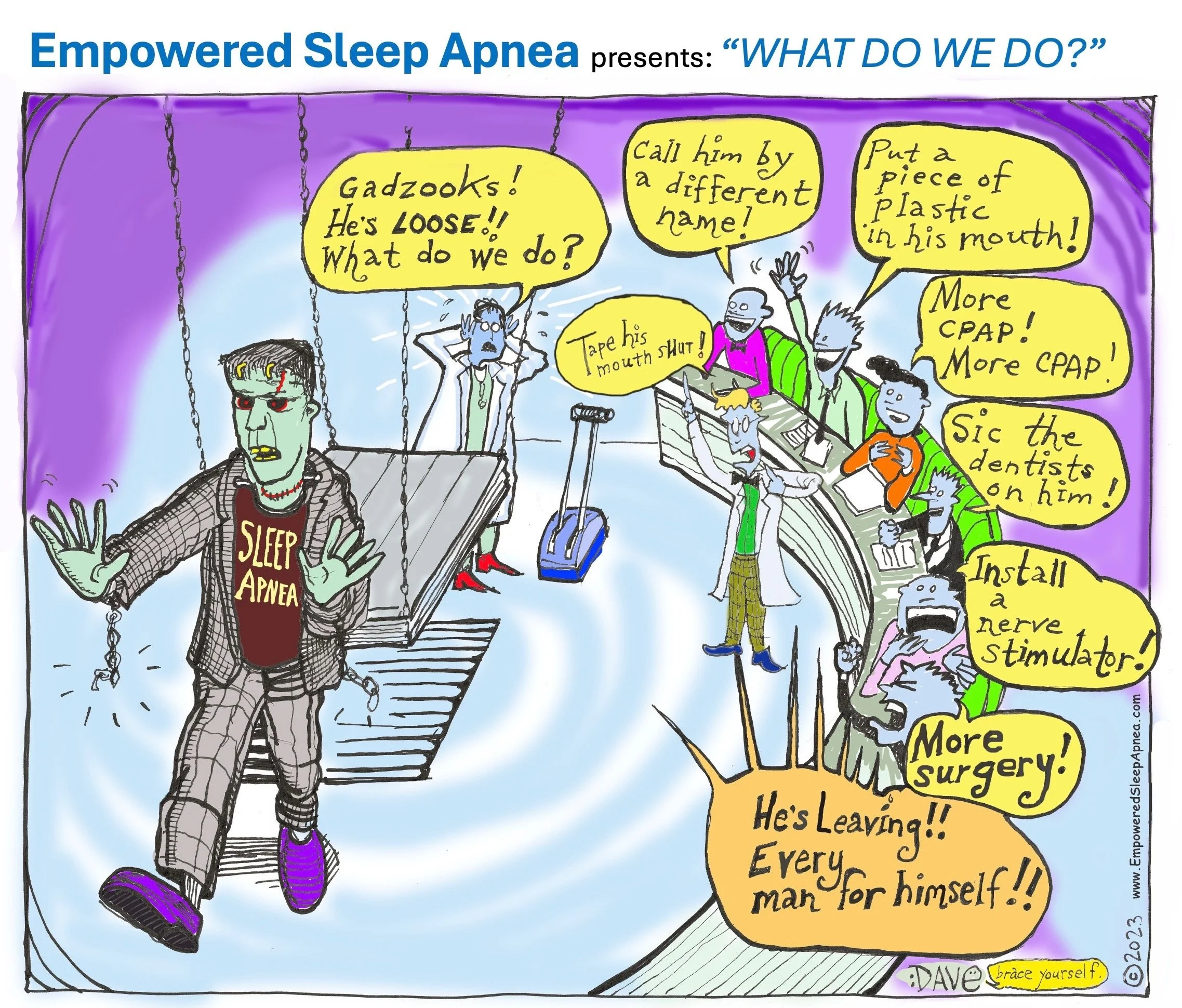
Empowered Sleep Apnea presents: “WHAT DO WE DO?” cartoon appearing in: McCarty DE.Happy 57th Birthday to the Beast Known as Sleep Apnea! OR: The Monster Has Left the Building. WHAT DO WE DO?Dental Sleep Practice magazine.5/19/23 [7] Different interpretations of the therapeutic implications of the label known as “Sleep Apnea” leads to a cacophony of voices with different versions of the truth…similar to what we see with “insomnia”
~ ~ ~ ~ ~
Modern insomnia research increasingly reflects this tension. Neurophysiological studies suggest that “insomnia” does not correspond to a single biomarker or unified disease entity. Individual physiological features demonstrate weak discriminatory value in isolation; meaningful classification emerges only through multivariate patterns distributed across multiple systems.[4] In other words, rather than representing a knowable disease entity, that thing we call “insomnia” is the final common pathway of manifold and distributed patterns of central nervous system activation and hyperarousal.[4]
This is a profoundly important development.
It suggests that insomnia isn’t a singular pathological object waiting to be discovered, but rather a family of unstable physiological states sharing overlapping phenomenology.
From this exercise, we see a practical truth emerge: the language of diagnosis remains useful as a starting point, but the underlying reality for problem-solving is process-oriented rather than categorical.
~ ~ ~ ~ ~
Changing the Game by Defining the Playing Field
The implications of this idea for clinical practice are substantial and game changing. When “insomnia” is approached primarily as a label, treatment can drift toward protocolized symptom management detached from mechanism. The therapeutic conversation narrows around the category itself:
Do we add medication?
Do we intensify CBT-I?
Do we combine therapies?
These are important questions, to be sure, and the guideline addresses them carefully and responsibly.[3] However, beneath these important questions lies a more fundamental inquiry:
What processes are destabilizing this patient’s sleep in the first place?
~ ~ ~ ~ ~
Structure for the Narrative
More than a decade ago, I proposed a “Five-Finger Approach” to problem-solving in clinical sleep medicine as a way of structuring this broader search[5] and have since advocated that this tool be shared collaboratively with our patients.[6] The framework organizes contributors to sleep-wake dissatisfaction into five interacting domains: circadian factors, pharmacologic influences, medical conditions, psychiatric and psychosocial factors, and primary sleep disorders.[5]
My goal was never to abolish diagnostic labels, which remain indispensable maps and reference points. Instead, the Five Finger Approach allows a structured (and, importantly, shared) method for unpacking the processes contributing to a nonspecific set of complaints.
Seen through this lens, “insomnia” becomes less a destination and more an entry point into an ongoing investigation, the clinician no longer asking merely whether the patient “has insomnia,” but iteratively (and collaboratively) digging into the interacting processes converging into the experience currently being given that name.
This shift may sound subtle, but clinically, it changes everything.
~ ~ ~ ~ ~
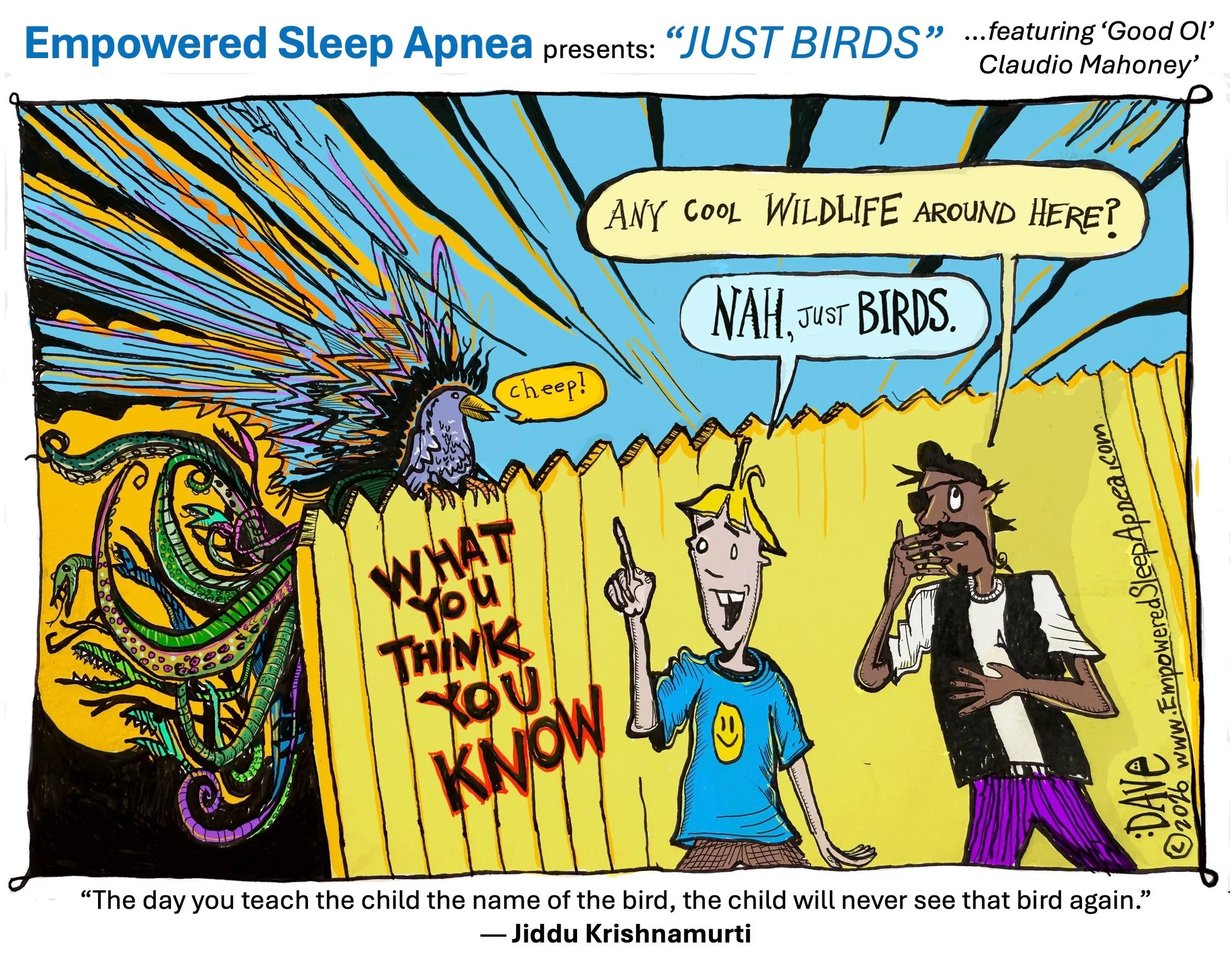
McCarty DE Empowered Sleep Apnea presents: “JUST BIRDS” appearing in: SLEEP REVIEW magazine, (coming soon, May 2026). [An earlier version of this cartoon appeared in: McCarty DE. The Tyranny of Labels. OR: Ode to the Nameless Bird. Published online 8/15/25 in: Dave’s Notes (official blog of Empowered Sleep Apnea)] [8]
~ ~ ~ ~ ~
Language and Human Behavior
The discussion of word choice isn’t just an exercise for word nerds, as I mentioned before.
Language matters because it directs attention. Words shape what clinicians search for and what patients come to believe about themselves. A term as broad as insomnia can inadvertently create the illusion of explanatory closure long before true understanding has occurred.
Writing during an era of ideological extremism and accelerating technological complexity, Korzybski understood this danger well. He worried that human beings were becoming hypnotized by abstractions detached from lived reality.[2] While his concerns extended far beyond medicine, the underlying principle feels strikingly contemporary.
Modern healthcare increasingly depends upon abstraction: Electronic medical records, ICD coding structures, treatment pathways, quality metrics, and evidence hierarchies all require compressing human complexity into manageable symbolic systems.
Again: this is not inherently bad, but Korzybski reminds us that every abstraction leaves something out. Every map omits granular terrain.
The AASM guideline itself tacitly acknowledges this reality. Its repeated emphasis on patient preference and individualized treatment decisions reflects a general recognition that no single pathway adequately captures the phenomenon we currently call “insomnia”.[3] Some patients prioritize total sleep time; others are more worried about daytime functioning. Some individuals fear medication exposure, while others seek rapid symptom relief despite tradeoffs.[3] Every case is as individual as a fingerprint.
In every instance, “treatment” becomes a negotiation between mechanisms, goals, risks, and meanings. In practice, we see that clinicians are already functioning as systems navigators whether they explicitly frame themselves that way or not.
Perhaps this is the deeper lesson Korzybski’s “General Semantics” project still offers modern medicine. It’s not anti-language or anti-science, by any means. It’s not an argument against the utility of having diagnostic categories.
Instead, I see it as a cry for epistemic humility, something Sleep Medicine could use a little sprinkle of, these days. It’s a reminder that our models, categories, and labels are clever representations of reality, but they’re not reality itself.
Sure, we’ve made some pretty useful maps and these can guide extraordinary clinical discoveries! However, when we mistake the map for the territory itself, we constrain our perceptive power, and our inquiry narrows. We inexorably morph into Osler’s grounded, port-bound sailor: knowledgeable but practically irrelevant for day-to-day navigation.
In closing, I’ll admit that “insomnia” is here to stay, and I’m OK with that. The word remains clinically useful and will undoubtedly persist. The point I’m making is that perhaps we’d all benefit from holding that word gently…not as an endpoint or a mandate to follow a specific treatment algorithm…but instead as a provisional marker pointing toward deeper physiological and psychological processes still requiring exploration.
As a doorway to discovery, the pirate in me is saying methinks that’ll work just fine!
I’ll again shout out that the new AASM guideline[3] represents a thoughtful effort to navigate an extraordinarily complex clinical landscape, and I’m grateful it’s out there. Its caution, flexibility, and emphasis on patient-centered care deserve recognition.
At the same time, the document unintentionally reveals the limitations of purely label-based thinking. The further one reads into its recommendations, the clearer it becomes that this thing we’re calling “insomnia” is not a singular disease entity at all, but instead an evolving, multidimensional process unfolding differently across individuals. In a word, it’s complex. I’m just recommending that we talk about it, that’s all. That realization may ultimately prove more important than any individual recommendation within the guideline itself.
A century ago, Korzybski warned about the confusion that begins when we mistake the map for the territory, while Osler observed the limitations of learning clinical practice solely from books.
Modern sleep medicine is bouncing up against these same lessons again.
So, gather ye maps, steady sea-mates!Read all ye can!
But be wary…keep your sea-legs about you…and look alive!When it comes to “insomnia,” there be stormy seas to navigate!
Methinks it’s time to start calling directions from topside!
Kind mojo and happy sailing,
Dave
David E McCarty, MD FAASM
Boulder, Colorado
10 May 2026
~ ~ ~ ~ ~
References
Osler W. Books and Men. In: Aequanimitas, with Other Addresses to Medical Students, Nurses and Practitioners of Medicine. Philadelphia: P. Blakiston’s Son & Co.; 1904.
Korzybski A. Science and Sanity: An Introduction to Non-Aristotelian Systems and General Semantics. Lancaster, PA: International Non-Aristotelian Library Publishing Company; 1933.
Buysse DJ, Arnedt JT, Buenaver L, et al. Combination treatment for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2026.
Christensen JAE, et al. Multivariate EEG-derived insomnia score reveals distributed neurophysiological patterns. Sleep. 2026.
McCarty DE. Beyond Ockham’s razor: redefining problem-solving in clinical sleep medicine using a Five-Finger Approach.J Clin Sleep Med. 2010;6(6):550–555
McCarty DE. The five finger approach to sleep-wake complaints (continuing education). Orthodontic Practice US. Fall 2023. 14(3),23-29
McCarty DE.Happy 57th Birthday to the Beast Known as Sleep Apnea! OR: The Monster Has Left the Building. WHAT DO WE DO?Dental Sleep Practice magazine.5/19/23
McCarty DE. The Tyranny of Labels. OR: Ode to the Nameless Bird. Published online 8/15/25 in: Dave’s Notes (official blog of Empowered Sleep Apnea)
Korzybski A. Science and Sanity: An Introduction to Non-Aristotelian Systems and General Semantics. 5th ed. Brooklyn, NY: Institute of General Semantics; 1994.