

(this is what EMPOWERED medicine looks like)
OR: How NARRATIVE-Based Medicine at Rebis Helps Clinicians Survive the Data Avalanche
~ ~ ~ ~ ~
By David E McCarty MD FAASM (…but you can call me Dave)
18 May 2026
~ ~ ~ ~ ~
“If you want to build a ship, do not drum up people to gather wood and assign them tasks and work, but rather teach them to long for the endless immensity of the sea.”
— commonly attributed to Antoine de Saint-Exupéry, author of The Little Prince
~ ~ ~ ~ ~
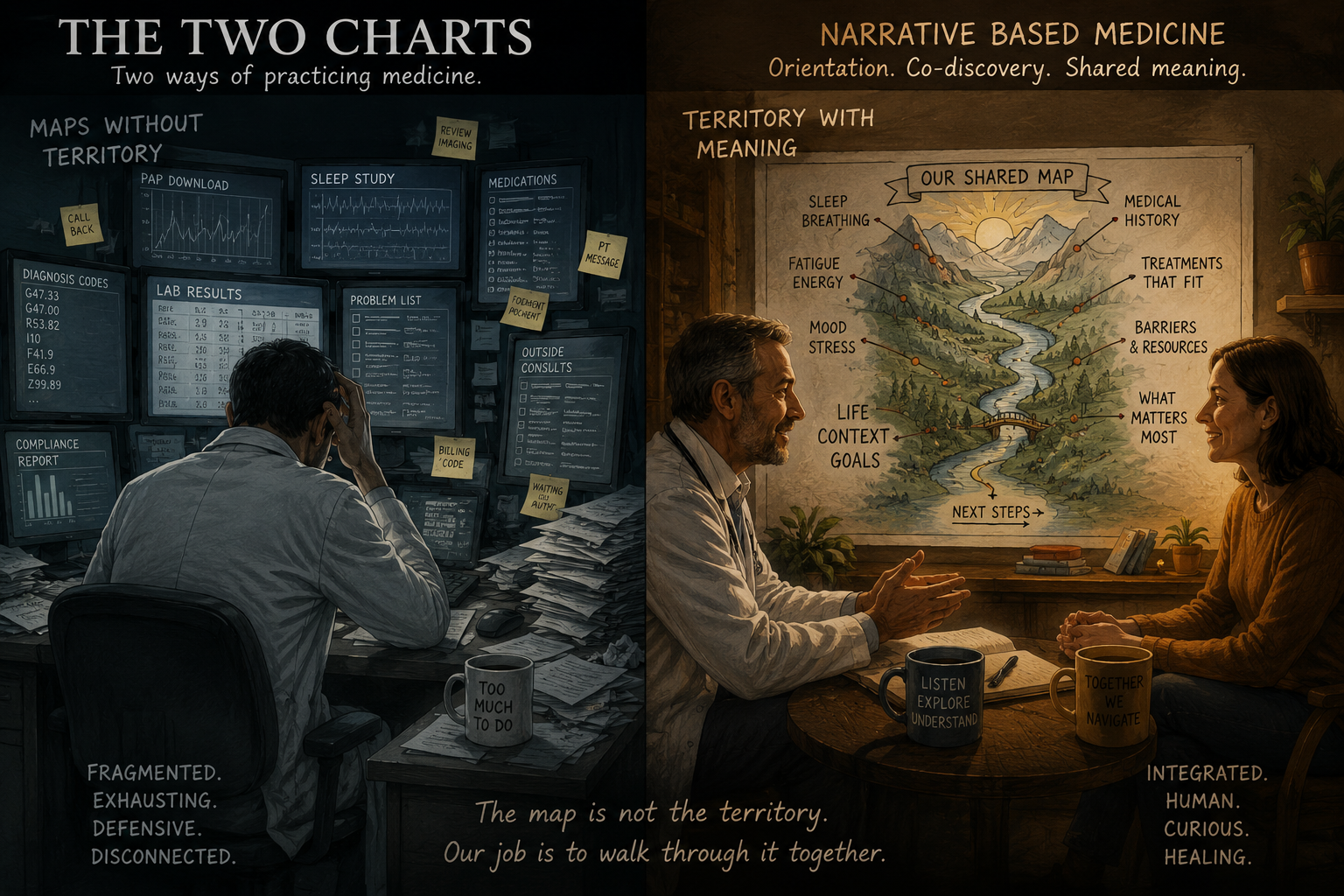
The map is not the territory…(image created collaboratively with ChatGPT)
A Day in the Life…
The morning alarm rings, and a day of clinical medicine lies ahead: How do you prepare for it? Is there a knot in your stomach? Do you feel the weight of your clinical EHR in-basket like a walnut in your throat?
Do you have that urge to get the chart pre-started…to get ahead of it all…so that all the information can be there, so the problem can be understood and quantified…so that you can be…READY??
If so, you’re not alone! Modern medicine has a fragmentation and information overload problem so profound, so normalized, and so deeply embedded into the emotional architecture of clinical training that most of us no longer recognize it as fragmentation at all. Instead, we maintain the self-destructive delusion that controlling the avalanche itself is somehow equivalent to professional rigor, responsibility, preparedness, and competence.
The modern clinician arrives at the encounter carrying a thousand disconnected maps:
Diagnosis codes.
Sleep study reports.
PAP downloads.
Medication lists.
Portal messages.
Radiology interpretations.
Laboratory values.
Outside consultations.
Problem lists.
Compliance reports.
Templates.
Algorithms.
Billing structures.
Quality metrics.
<<…SIGH!!!…..>>
Useful bits of data, useful maps, every one of them! An observation, though: none of them is the thing-in-itself. None of them is the actual territory.
Alfred Korzybski, the founder of General Semantics, famously warned that "the map is not the territory," a deceptively simple phrase that turns out to contain an almost frightening degree of relevance to the current state of healthcare, where patients increasingly experience themselves not as "known human beings" moving through time with evolving stories and changing needs, but as collections of fragmented abstractions loosely stapled together inside the electronic medical record.[1]
Dr. Kurt Stange articulated this foundational problem beautifully in his 2009 editorial message called The Problem of Fragmentation and the Need for Integrative Solutions. In this piece, Stange described modern healthcare systems as increasingly focused on "the parts without adequately appreciating their relation to the evolving whole." The phrase "evolving whole" matters here, because it points directly toward the thing modern medicine keeps accidentally amputating from the clinical encounter: the living, emerging, and complex human story.[2]
~ ~ ~ ~ ~
Enter: NARRATIVE
You'll hear me using the word "NARRATIVE" a lot, around the Empowered Sleep Apnea project, and in the halls of Rebis Health.
Around here, NARRATIVE doesn't mean "storytelling" in the sentimental sense—we're not talking about endless meandering autobiography or unstructured emotional catharsis! Around here, NARRATIVE has a structure, and orienting around that structure helps the patient, the clinicians, and the administrative and telephone staff share a vision for what we are ultimately trying to accomplish, which is a healing journey, centered around the patient.
Around here, embedded in the word NARRATIVE is that whole “complexity-sensemaking machine”! NARRATIVE is an information-processing architecture designed to help human beings navigate complexity without becoming crushed beneath it.
Folks, that distinction matters so much, we consider it to be foundational to Team Rebis' success!
Modern medicine often behaves as though the primary task of the clinician is to absorb and synthesize an impossible volume of fragmented information before entering the room, creating the strange and exhausting expectation that the patient should somehow already be understood before the first handshake occurs, as though enough pre-charting might finally abolish uncertainty once and for all. The emotional result of this approach is familiar to nearly every healthcare worker alive: anticipatory dread, compulsive preparation rituals, defensive documentation, cognitive overload, depersonalization, burnout, and the creeping sensation that one is slowly becoming less healer than air traffic controller for an endless stream of disconnected pathology.[3][4][5]
None of this is accidental, folks. The sensation that fragmented systems create more work is not an illusion. They do!
Fragmented systems create fragmented emotional lives, serving as an additional barrier to sensemaking of complexity, especially when the problem-solving necessarily crosses silos.
The syndrome of emotional exhaustion, depersonalization, and diminished personal accomplishment known as Physician Burnout now exceeds 50% prevalence in studies of both trainees and practicing physicians, and its drivers are largely rooted within healthcare organizations and systems: excessive workloads, inefficient work processes, clerical burdens, and lack of physician input or control.[3]
Electronic health record use has been identified as a significant contributor, with a recent meta-analysis of 41 studies encompassing over 54,000 healthcare professionals finding that EHR use was associated with a 2.5-fold increased risk of occupational burnout (OR = 2.49; 95% CI, 1.82–3.41), driven primarily by poor system design, excessive documentation time, and heavy administrative burdens.[6] The Association of Electronic Health Record Design and Use Factors with Clinician Stress and Burnout study identified seven specific EHR-related stressors—including inf ormation overload, note bloat, notes geared toward billing rather than patient care, and interference with the patient-clinician relationship—each significantly associated with validated measures of stress and burnout.[7]
~ ~ ~ ~ ~
You arrive at clinic, curious.
That's the first thing you notice.
Curiosity.
You’re not armored, not bracing for combat with the chart.
You’re not trying to memorize twelve strangers before meeting them.
You’re curious.
The schedule feels less like an avalanche and more like a neat collection of unopened parcels, brown-paper-packages-tied-up-with-string sort of parcels.
You wonder who these people are.
You wonder what parts of themselves have been compressed into labels before arriving here.
OSA.
Insomnia.
CPAP failure.
Anxiety.
Noncompliant.
Maps.
Always maps.
None of this bothers you at all, because you know your footing, and reading maps is what you do well.
You get a twinge of butterflies in your stomach (as you always do) when you greet the patient and bring him back.
This is going to be fun!
~ ~ ~ ~ ~
The Rebis ecosystem was built around a simple but increasingly radical proposition: human beings make better decisions when they understand the terrain they are standing in, which means that complexity must be co-managed and co-discovered rather than dictated from above.
Shared decision-making (a collaborative approach incorporating the active involvement of patients in decisions concerning their care) is supported by over 100 randomized trials demonstrating improved patient understanding, acceptance, satisfaction, and involvement in medical decisions.[8] An umbrella review of 48 systematic reviews found that shared decision-making implementation did not typically increase costs or consultation time while producing neutral to positive benefits on outcomes and quality.[9]
At Rebis, our process begins with what we call AWAKEN, though the word itself can be misleading if interpreted too narrowly, because AWAKEN is not merely a "New Patient Visit." AWAKEN is an orientation process part of the journey, a ritualized return to the patient's lived experience that occurs every single time the patient enters the clinical space, regardless of whether the encounter is the first visit or the fiftieth.
The structure itself is surprisingly simple.
First: orientation to the system. Second: the Self-Reported Sleep Satisfaction Score. Third: exploration of pain points. Fourth: hypothesis testing for root causes using the Five Finger Approach. Fifth: territory investigation and complexity deconstruction of that thing we call "Sleep Apnea," understood here not as a rigid identity-label but as…
…unstable breathing during sleep that negatively impacts health and well-being, expressed through two major physiologic flavors—obstructive and central instability—each containing many moving parts.[10][11]
The sequence on this roll-out matters because it protects curiosity for both clinician and patient, from the beginning of the process and extending throughout, allowing iterative co-discovery.
Traditional history-taking often collapses under what might best be described as "jargon-avalanche syndrome," where the clinician attempts to establish mastery over the encounter through anticipatory abstraction, rapidly converting the patient into a diagnostic object before sufficient orientation to the lived experience has occurred.
Ilgen, Eva, and Regehr have argued that diagnosis in medicine aspirationally represents not merely the assignment of a label (i.e.: a solution at a single point in time) but a dynamic process of "making meaning" from data that are intrinsically dynamic, experienced idiosyncratically, and rich with opportunities for exploration.[12]
Rebis' model of Narrative Based Medicine deliberately reverses the traditional sequencing by systematizing the order: human signal arrives first; the abstractions arrive later.
That reversal changes everything.
~ ~ ~ ~ ~
Two minutes before the encounter, you open the chart.
Not twenty minutes.
Two.
You orient yourself. Who sent them? What kinds of data exist? What major landmarks are already visible in the terrain?
Maybe there's a PAP download…
…perhaps a home sleep study…
…a cone beam CT?
…and stack of old records from another system...
You notice them, the way a seasoned river rafter notes how high the water is running, and the size of the rocks that lay downstream. You have enough experience to know what to do with the obstacles when you get there, so you don't have to run the whole river beforehand.
You know better than that.
A quick review of essentials is what's needed, and you know the raft is ready to roll.
That restraint matters more than it first appears.
The patient has not entered the room yet, so the territory you're really interested in has not yet revealed itself.
The game’s afoot!
The patient enters the room…
~ ~ ~ ~ ~
The patient arrives already carrying a diagnosis of "Sleep Apnea," already wearing the emotional posture of someone expecting a transactional equipment-renewal encounter, already assuming the visit will revolve around machine settings, insurance qualifications, compliance metrics, and the familiar industrial choreography of modern durable medical equipment culture.
You smile because you are genuinely glad he came.
"Welcome to Team Rebis," you say. "We do things a little differently around here."
The patient braces slightly, though only slightly.
"We practice a style of medicine called Narrative Based Medicine. That means this really is all about you. Our job is simply to help structure the search."
The room softens, a tiny bit, a microscopic shift; it’s almost invisible.
~ ~ ~ ~ ~
This is a Rebis moment; this shift is small, hard to see, but foundationally important.
See, at Rebis, the first task is not diagnosis; the first task is orientation.
~ ~ ~ ~ ~
"How satisfied are you with your current sleep-wake experience?"
The patient pauses.
"Maybe…seven out of ten."
Now the encounter begins.
"Tell me where the points went."
That question changes the emotional geometry of the room because the patient is no longer defending a diagnosis or attempting to satisfy the implicit expectations of a specialist encounter. The patient is now exploring lived experience in real time with another human being.
"The mask wakes me up."
"I'm less sleepy driving."
"My wife says the snoring is better."
"I still don't feel rested."
The NARRATIVE begins emerging organically from the territory itself, and all of it is relevant.
~ ~ ~ ~ ~
Patient-Centered Care Means…Involving the Patient
Seems we didn’t come up with this idea.
Starting from the patient's viewpoint is based on solid contemporary problem-solving science. The whole idea is to have a system that captures the patient’s voice and engages them in medical decision-making.
A Cochrane review of 116 randomized controlled trials (N = 49,785) found that implementing PROMs improved diagnosis and documentation (RR = 1.73; 95% CI, 1.44 to 2.08) as well as communication between healthcare professionals and patients (SMD = 0.36; 95% CI, 0.21 to 0.52).[13]
PROMs facilitate shared decision-making and guide self-management by engage patients, caretakers, and clinicians in care.[14]
Rebis and the structure of our NARRATIVE-based model make this aspirational goal systematically achievable, and shared across the system.
~ ~ ~ ~ ~
Now, you’ve got your numeric score, which opened a discussion about “pain points.”
Now you're ready to start snooping around, to engage your curiosity with the search: "What could be causing this?" is the relevant question, and you call attention to it. You've already used your reflective listening skills to fact-check what you think you understand about their NARRATIVE:
"Let me get this straight: you're saying you've got 7/10 sleep-wake satisfaction, with points lost due to awareness of the mask and pressure, dry mouth in the morning, and yawning all afternoon, without dozing off? Is that right?"
You've verified together (you can call it "co-discovery", if you like!) the reality of what the two of you are working on.
Then you take that NARRATIVE to "The Hand".
You take it to the Five Finger Approach, and you do a little digging.
~ ~ ~ ~ ~
The Five Finger Approach is a Shared Hypothesis Generating Machine
ENTER: The Five Finger Approach (FFA)--not as some sort of checklist, but as a strategic collaborative hypothesis-testing structure openly shared with the patient.[15]
Think of it as five rooms to check out, to see if the bank robber is in there: Circadian rhythm. Pharmacologic contributors. Medical contributors. Psychological and environmental contributors. Primary sleep diagnoses. We, the experts, ask questions and look for historical, physical and physiologic evidence for the problems hiding in these five domains, that might explain where the points went. That's what we do.
Here's the fun part: at Rebis, we share the structure of our investigation with our patients! Transparency matters enormously here because hidden complexitycreates fearwhileshared complexity creates orientation.
Here is where vibrational orientation matters: our stance is curious, probing. After all, our patient is being welcomed into the cognitive architecture of the clinic itself, to be allowed to see how the system thinks, to be allowed to participate in the meaning-making process. This is no longer about waiting passively for “The Expert” to emerge from the cave carrying “The Correct Answer.” This is about relational engagement.
Schwartzstein and Iyer posited that medical education has historically overemphasized pattern recognition (label-based care) and underemphasized pathophysiological reasoning (iterative whole-being care). The next level in patient care (they argue) is for clinicians to develop what they call "adaptive expertise," which can be defined as flexibly creating solutions rather than forcing problems into familiar categories.[16] Any of this sound familiar?
There’s not much published about this, but there’s some signal that’s worth talking about. A systematic review and meta-analysis of cognitive reasoning tools found that structured approaches to diagnostic reasoning led to small but clinically important improvements in diagnostic accuracy (Hedges' g = 0.20; 95% CI, 0.10 to 0.29; p 0.001).[17]
Cognitive biases (including premature closure, anchoring, and overconfidence) have been associated with diagnostic inaccuracies in 36.5% to 77% of case scenarios, and instruction in metacognition and structured reasoning has the potential to reduce diagnostic errors and improve patient safety.[18][19] Of note, the FFA was specifically created as a countermeasure to early closure, and is functionally an iterative way to protect the patient’s story. [15]
~ ~ ~ ~ ~
After you introduce the patient to the Five Finger Approach as a tool to understand their NARRATIVE, you have that moment that all Rebis clinicians have come to love: the moment when the lights come on…the moment when the patient begins making connections spontaneously…
"So maybe the CPAP isn't the whole story?"
Exactly.
Now we're thinking together, you think to yourself, as you smile.
Now we are navigating territory, rather than worshipping maps.
~ ~ ~ ~ ~
The Vibe of Empowerment
The remarkable thing about practicing this way is how much lighter medicine begins to feel once the clinician stops attempting to carry the entire avalanche alone!
Documentation becomes easier because sense-making has already communally occurred. Patient-Portal work burden decreases because decision-making nodes were shared transparently during the encounter itself. Patients become less frightened because the structure creates predictability and orientation.
There’s anthropology behind all this vibe-talk: turns out that fear in the decision-making territory makes us less effective as healers and makes our workplace potentially more toxic. Diagnostic uncertainty imposes a psychological threat on individuals' need for control and understanding, and patients tend to adopt compensatory behaviors to regain control in the face of that uncertainty.[20] Putting a face to those treading these worn floors, these are the irate, the angry, the cancel-culture denizens, trying desperately to get their power back. Sometimes a one-star Google review seems to be the only tool available.
At Rebis, we believe that if we engage our patient in a shared framework for the uncertainties we face, we experience a more collaborative and transparent environment. The literature would back up this assertion: a qualitative study developing a framework for communicating diagnostic uncertainty found that acknowledging uncertainty has potential benefits including strengthening clinician-patient relationships and trust, promoting better patient engagement, and advancing shared decision-making.[21]
Finally, in an empowered, spontaneous clinic, clinicians are simply less exhausted! Shared curiosity replaces defensive omniscience, and perception of work stress goes down. All of this is good for the longevity of our clinicians, as well as the clinic we work in!
This is not hand-wavey Pollyanna talk: a systematic review of 55 narrative medicine programs found evidence of high participant satisfaction and pre-post improvement in competencies such as relationship-building, empathy, confidence, and clinical skills, with an average of 88.3% of participants agreeing the program had positive outcomes; this also likely improves work satisfaction: qualitative evaluation further identified improvement in resilience and burnout detection and mitigation for the clinicians doing the work.[22]
With a NARRATIVE-grounded structure, the work becomes strangely joyful again.
This is not because complexity has vanished; it's because it finally has a navigable structure.
~ ~ ~ ~ ~
To Seek Clarity or Deploy Change?
The visit ends, as it often does, with only a few meaningful questions remaining.
Do we need more information for clarity?
If yes, the patient proceeds toward some version of the Rebis CORE ASSESSMENT, a precision-medicine snapshot of anatomy, physiology, form, and function designed to clarify the moving parts contributing to the patient's NARRATIVE.
This clarity is vitally needed, now that we know that this beast we go around calling "Sleep Apnea" is not just "one thing." Indeed, there's a growing appreciation that the underlying etiology ("endotype") and clinical manifestation ("phenotype") of OSA in an individual are impossible to capture with the AHI alone.
At Rebis, we believe that treatment should be individualized on the basis of the underlying cause of Sleep Apnea (two flavors of instability of breathing during sleep that may impact health; many moving parts in each flavor…), and we want our patients to understand which symptoms and outcomes will respond to treatment and by how much.
Why go to this trouble? Because not all AHI's are equal, and there is no "one size fits all" solution! Cluster analysis studies have identified symptom-based subtypes such as "excessively sleepy" and "disturbed sleep" with differing impact of CPAP on symptoms and health-related quality of life. We can also stratify the risk the disease poses by using objective measures such as hypoxic burden, arousals, or both, patterns in which show varying risks of cardiovascular disease and response to therapy.[10]
If we agree that this “thing” we call “Sleep Apnea” is complex (it is!) and has “many moving parts” (it does!), we have to re-imagine what a proper snapshot of those moving parts will look like. When we have language to talk about the developmental and craniofacial “moving parts” of Sleep Apnea, the conversation may materially change, depending on the NARRATIVE. The point here is to have a step in the process that allows a measured assessment of where this complex problem stands, and it must allow a larger picture than the AHI.
The next question to be reckoned with: should change the therapeutic pathway? At Rebis, this is a shared decision, based on mutually understood goals, using the Five Reasons to Treat paradigm as the structured framework. Should we change therapy? Only if it will have a positive impact on one of the Reasons that matters to the patient!
If the answer is yes, the intervention is approached as a shared “N-of-1 experiment” in the spirit of evidence-based medicine founder David Sackett, complete with individualized goals, explicit discussion of risks and tradeoffs, clearly defined follow-up metrics, and a collaborative plan for assessing whether the change actually improved the patient's lived experience.
Should we try a lower PAP setting, as a comparison trial? What would we be trying to accomplish with the change? How will we know if we’re successful? What could go wrong? How will we follow up? You get the idea. Precision medicine requires a shared language and shared understanding for the complexity of the problem at hand.
What's an N-of-1 trial? It's an individual treatment plan of "A" vs "B"! The idea is that, for an individual patient, this precision tuning is more rigorous than a systematic review of multiple RCTs for making evidence-based treatment decisions for individual patients. Think about it and it makes sense: it's the best way to clinically estimate individual treatment effects, rather than extrapolating "the best treatment" from population averages.[23] A review of over 2,154 single-patient trials across 108 studies found that N-of-1 designs facilitate finely graded individualized care, enhance therapeutic precision, and may reduce costs.[24]
The entire structure of Rebis’ take on NARRATIVE-based medicine ultimately revolves around one central philosophical recognition, bringing us back to one of the first points made in this piece:
The map is not the territory.[1]
The patient is not the chart; the diagnosis is not the person.
Human beings are the territory.
Our job is to walk through it together.
~ ~ ~ ~ ~
You're finishing up your last patient of the day: it's a same-day add-on for someone who opted in to a spot that opened due to a late cancellation. In your old job, this would have stressed you out, because you didn't have any time to prepare. Here at Rebis, it's just a late-arriving guest to a well-constructed party, and you're happy to facilitate.
It didn't take you long to understand the NARRATIVE. You established the pain points, you poked around the Five Finger Approach to see that this fella almost certainly has Sleep Apnea, and it's probably bad.
You're find yourself feeling proud of your team and your system, because we were able to get him in and on board, so quick, so effortlessly. You're really glad you don't live under the mountain of data avalanche anymore.
You introduce your new patient to the Five Reasons to Treat, and agree that you'll table the complex discussion about RISK until next time, when you can review his sleep study results. It's a big world, and there's lots to learn. There will be plenty of time to revisit this at his EMPOWER visit, so you don't stress over it.
As you conduct your root cause search, you also introduce the patient to the structure of the Five Finger Approach. You know that when he understands there is a structure to how we talk about these things, he'll become less fearful.
You comment on some of the other domains where there may be opportunities for work later, but you don't stress it too much. You have a sense of timing. You don't overload the patient. The breathing is foundational (you both agree about that), so it's agreed that's where you'll start. The patient's fully on board. You feel reassured by this, because you know if there's something not right, if it's important, it will come back.
The NARRATIVE-based structure assures us of that, whether it's with you or with someone else. It’s built into the structure.
You smile. You know the system has got this!
You close the day without much charting to do. Your robotic Ambient Note Taker has written down your co-discovery conversations in real-time, and you've gotten pretty good at summing everything up in the Rebis format for the H & P:
NARRATIVE
Five Finger breakdown
Five Reasons breakdown
Specific plans.
BOOM! Easy-Peasy! You're proud of this little nugget of complexity-deconstruction that you can share with your team-mates in the larger ecosystem! You know that this section of the chart documentation is the lifeblood of the team, because it allows anyone on the team to open the chart to the most recent clinical encounter, and decode the complexity with a language that we all can share.
You take pride in the way you capture all of it, so succinctly, the way a banzai tree artist lives for the “perfecting snip.”
There.
Done.
You close your laptop and power down, tired but happy.
You know the system has got this…
…and that night, you sleep…just like a baby.
~ ~ ~ ~ ~
That’s all I have, Life-Fans! In closing, I’ll just reflect that perhaps the real work of cultural transformation in medicine has less to do with forcing people into new workflows, and is more about helping them rediscover what they were longing for in the first place.
Maybe that’s why the old Saint-Exupéry line keeps rattling around in my head lately, the one about teaching our shipbuilders to long for the sea. At the end of the day, we don’t need to teach clinicians how to gather wood more efficiently.
We need to help them see the sea again.
Kind mojo,
Dave
David E McCarty MD FAASM
Longmont Colorado 18 May 2026
~ ~ ~ ~ ~
For my new team at Rebis as we build what Medicine can be
And for Tani, Erica and Sarah
For whom I wish I had discovered this language long ago
~ ~ ~ ~ ~
David E McCarty MD FAASM is the co-creator (with Ellen Stothard PhD) of the Empowered Sleep Apnea project (www.EmpoweredSleepApnea.com) and is the Chief Medical Officer of Rebis Health (www.RebisHealth.org).
References
[1] Korzybski A. Science and Sanity: An Introduction to Non-Aristotelian Systems and General Semantics. 5th ed. Englewood, NJ: Institute of General Semantics; 1994.
[2] Stange KC. The problem of fragmentation and the need for integrative solutions. Ann Fam Med. 2009;7(2):100-103. doi:10.1370/afm.971
[3] West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-529. doi:10.1111/joim.12752
[4] Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195-205. doi:10.1001/jamainternmed.2016.7674
[5] Tutty MA, West CP, Dyrbye LN, et al. Moral distress and occupational burnout in US physicians. JAMA Netw Open. 2026;9(3):e263161. doi:10.1001/jamanetworkopen.2026.3161
[6] Yang Y, Shi R, Wang Z, et al. Electronic health records-related determinants of healthcare professionals' burnout and mitigation strategies: systematic review and meta-analysis. Front Public Health. 2026;14:1751521. doi:10.3389/fpubh.2026.1751521
[7] Kroth PJ, Morioka-Douglas N, Veres S, et al. Association of electronic health record design and use factors with clinician stress and burnout. JAMA Netw Open. 2019;2(8):e199609. doi:10.1001/jamanetworkopen.2019.9609
[8] Dennison Himmelfarb CR, Beckie TM, Allen LA, et al. Shared decision-making and cardiovascular health: a scientific statement from the American Heart Association. Circulation. 2023;148(11):912-931. doi:10.1161/CIR.0000000000001162
[9] Bruch JD, Khazen M, Mahmic-Kaknjo M, Légaré F, Ellen ME. The effects of shared decision making on health outcomes, health care quality, cost, and consultation time: an umbrella review. Patient Educ Couns. 2024;129:108408. doi:10.1016/j.pec.2024.108408
[10] Edwards BA, Redline S, Sands SA, Owens RL. More than the sum of the respiratory events: personalized medicine approaches for obstructive sleep apnea. Am J Respir Crit Care Med. 2019;200(6):691-703. doi:10.1164/rccm.201901-0014TR
[11] Zinchuk A, Yaggi HK. Phenotypic subtypes of OSA: a challenge and opportunity for precision medicine. Chest. 2020;157(2):403-420. doi:10.1016/j.chest.2019.09.002
[12] Ilgen JS, Eva KW, Regehr G. What's in a label? Is diagnosis the start or the end of clinical reasoning? J Gen Intern Med. 2016;31(4):435-437. doi:10.1007/s11606-016-3592-7
[13] Gibbons C, Porter I, Gonçalves-Bradley DC, et al. Routine provision of feedback from patient-reported outcome measurements to healthcare providers and patients in clinical practice. Cochrane Database Syst Rev. 2021;10:CD011589. doi:10.1002/14651858.CD011589.pub2
[14] Noonan VK, Lyddiatt A, Ware P, et al. Montreal Accord on Patient-Reported Outcomes (PROs) use series—Paper 3: patient-reported outcomes can facilitate shared decision-making and guide self-management. J Clin Epidemiol. 2017;89:125-135. doi:10.1016/j.jclinepi.2017.04.017
[15] McCarty DE. Beyond Ockham's razor: redefining problem-solving in clinical sleep medicine using a "Five-Finger" approach. J Clin Sleep Med. 2010;6(3):292-296.
[16] Schwartzstein RM, Iyer AA. Critical thinking for 21st-century medicine—moving beyond illness scripts. JAMA. 2025;334(17):1509-1510. doi:10.1001/jama.2025.14901
[17] Staal J, Hooftman J, Gunput STG, et al. Effect on diagnostic accuracy of cognitive reasoning tools for the workplace setting: systematic review and meta-analysis. BMJ Qual Saf. 2022;31(12):899-910. doi:10.1136/bmjqs-2022-014865
[18] Saposnik G, Redelmeier D, Ruff CC, Tobler PN. Cognitive biases associated with medical decisions: a systematic review. BMC Med Inform Decis Mak. 2016;16(1):138. doi:10.1186/s12911-016-0377-1
[19] Royce CS, Hayes MM, Schwartzstein RMTeaching critical thinking: a case for instruction in cognitive biases to reduce diagnostic errors and improve patient safety. Acad Med. 2019;94(2):187-194. doi:10.1097/ACM.0000000000002518
[20] McKoane A, Sherman DK. Diagnostic uncertainty in patients, parents, and physicians: a compensatory control theory perspective. Health Psychol Rev. 2023;17(3):439-455. doi:10.1080/17437199.2022.2086899
[21] Khazen M, Mirica M, Carlile N, Groisser A, Schiff GD. Developing a framework and electronic tool for communicating diagnostic uncertainty in primary care: a qualitative study. JAMA Netw Open. 2023;6(3):e232218. doi:10.1001/jamanetworkopen.2023.2218
[22] Remein CD, Childs E, Pasco JC, et al Content and outcomes of narrative medicine programmes: a systematic review of the literature through 2019. BMJ Open. 2020;10(1):e031568. doi:10.1136/bmjopen-2019-031568
[23] Davidson KW, Silverstein M, Cheung K, Paluch RA, Epstein LH. Experimental designs to optimize treatments for individuals: personalized N-of-1 trials. JAMA Pediatr. 2021;175(4):404-409. doi:10.1001/jamapediatrics.2020.580
[24]Duan N, Kravitz RL, Schmid CH. Single-patient (N-of-1) trials: a pragmatic clinical decision methodology for patient-centered comparative effectiveness research. J Clin Epidemiol. 2013;66(8 Suppl):S21-S28. doi:10.1016/j.jclinepi.2013.04.006