

What’s In A Name? OR: What should “ORTHODONTICS” be called, anyway?
(…and why does it matter?)
~ ~ ~ ~ ~
By Kevin Boyd, DDS, MSc
&
David McCarty, MD, FAASM
(…but you can call me Dave)
23 March 2026
~ ~ ~ ~ ~
“Nominibus mollire licentiam.” *
— Cicero, De Officiis, c. 44 BCE
* By softening the name, we make the act permissible.
~ ~ ~ ~ ~
Sing it, Cicero! The NAMING of things has been important for aeons…
In the mid-1980s, a young woman in New England sought help for a problem that had defined much of her adolescence and early adulthood: relentless headaches that had begun shortly after orthodontic treatment at age thirteen.[1]
During that treatment, two of her upper lateral incisors—one small and malformed, the other removed for symmetry—were extracted. Her front teeth were then pulled backward to close the spaces. At the time, this was considered a routine orthodontic strategy.
Years later, still suffering, she consulted orthodontist William Hang, DDS, MSD. She asked him to do something that ran against conventional wisdom: reopen the spaces where her teeth had been removed and restore what she believed had been taken away.
According to Dr. Hang’s account, he initially told her it couldn’t be done. But after years of additional training and reconsideration, he ultimately agreed to try. The spaces were reopened, the missing teeth were replaced, and her headaches resolved.[1]
It is a striking story—not because it provides any scientific evidence whatsoever about causation, but because it elicits a question some of us might rarely stop to ask:
Why do we remove healthy teeth in children in the first place?
It gives one pause to consider it: these were not diseased teeth. These were not fractured teeth.
These were healthy, living teeth.
The answer is so practical, that it, again, gives one pause. We remove teeth to make room, to relieve crowding and allow adjacent teeth to be aligned for an aesthetically pleasing arrangement, like little soldiers standing at attention. Orthodontics, after all, is commonly understood as “the specialty that straightens (ortho) teeth (dontics).”
We agree that straight teeth are nice, and a pretty smile should be a goal for all of us. But what if the “straight teeth” part is just the beginning?
And…walk with us here…what if the name of the specialty itself is part of the problem?
~ ~ ~ ~ ~
When the name defines the work
As we mentioned above, the word orthodontics comes from the Greek orthos (straight) and odous (tooth). Straight teeth. The name does exactly what names are supposed to do: it tells the public, insurers, and even practitioners what the field is about.
The problem is that teeth are not isolated objects. They sit within an interconnected craniofacial and respiratory complex (CFRC) that includes the face, jaws, tongue, airway corridors—including the nasal cavity, sinuses and throat—and muscles of breathing and posture. Decisions that cause change to the size or shape of that system can have good or bad consequences extending far beyond the smile.
When we think only in terms of straight teeth, we risk losing sight of the larger biological mission: guiding optimal CFRC development so that we can best interact with and adapt to our environment. Architects have long understood that function follows form. Turns out the geometry of our face is something that develops as we grow, and the way we habitually chew, breathe, and swallow plays a foundational role in all of it.
All of this means that the teeth aren’t a symptom to be managed.
They’re a marker.
Through this lens, the teeth are not the problem but are instead often the visible casualties of something deeper.
This concern is not new, nor is it coming from outside the profession.
As it went down in that iconic horror film: the call came from inside the house…[2]
~ ~ ~ ~ ~
A warning from inside orthodontics
In 1998, David C. Hamilton, DDS, MS, published an editorial in the American Journal of Orthodontics and Dentofacial Orthopedics titled “The Emancipation of Dentofacial Orthopedics.”[3] Writing to his peers, Hamilton argued that the highest calling of any health profession is the prevention of disease or deformity—and that orthodontics had drifted away from this goal.
He emphasized that early facial and skeletal orthopedics, when appropriately applied, could prevent the later development of “dentofacial dysplasia”—a concept that parallels what Mew later described as craniofacial dystrophy.[4] Both terms describe incomplete development to full genetic potential of the hard and soft tissues comprising the intimately connected jaws, face, and airway network—the maxilla, mandible, nasal airspace, and their autonomic integration. Hamilton cautioned even back then that economic pressures and cultural habits were quietly shaping treatment decisions.
Most importantly, he urged the profession to recognize what it truly was:
“Orthodontists must entertain a paradigm shift… and recognize that they are in the business of facial orthopedics.”
That sentence is almost three decades old; yet culturally, orthodontics remains framed almost entirely as a cosmetic dental service.
The result is a mismatch between what the specialty can influence and what it is publicly understood to do.
~ ~ ~ ~ ~
The cost of a narrow frame
When a field is defined narrowly, its ethical horizon narrows with it.
If orthodontics is “about teeth,” then extracting healthy teeth to straighten a smile can seem like a reasonable trade. But if orthodontics—especially dentofacial orthodontics—is fundamentally about guiding craniofacial and respiratory growth …
…i.e.: preserving the structural foundations for breathing, sleep, and long-term health…
…then those same decisions demand a different level of scrutiny.
From our respective vantage points in sleep medicine and craniofacial-respiratory development, we increasingly see “former children” (a.k.a.: “adults”) struggling with downstream problems: sleep-disordered breathing, temporomandibular jaw-joint dysfunction, chronic fatigue, and difficulty tolerating standard therapies. Often, buried in their histories, is orthodontic treatment that reduced oral and respiratory space during key developmental years. This does not establish direct causation, but it raises legitimate biological questions about how space, structure, and airway development intersect.
This does not mean orthodontists are careless or incompetent; it simply means we’ve all been working inside an academic and clinical practice framework that’s inadequately matched to the awesome responsibility for it carries.
~ ~ ~ ~ ~
Why words matter
Names are not just labels; they are signals. They shape training priorities, referral patterns, insurance coverage, and public expectations. Perhaps most importantly, they influence what clinicians notice—and what they overlook.
When a specialty is named for its most visible output rather than its deepest function (and responsibility) it risks becoming very good at the former while neglecting the latter. Coincident with David Hamilton’s AJO/DO invited editorial, the healthcare discipline of Orthodontics reached that inflection point in 1998—and we are well past it now. If the field’s true mission includes guiding facial growth, optimizing and preserving naso-respiratory health, and preventing downstream disease, then its name should reflect that reality.
~ ~ ~ ~ ~
A proposal
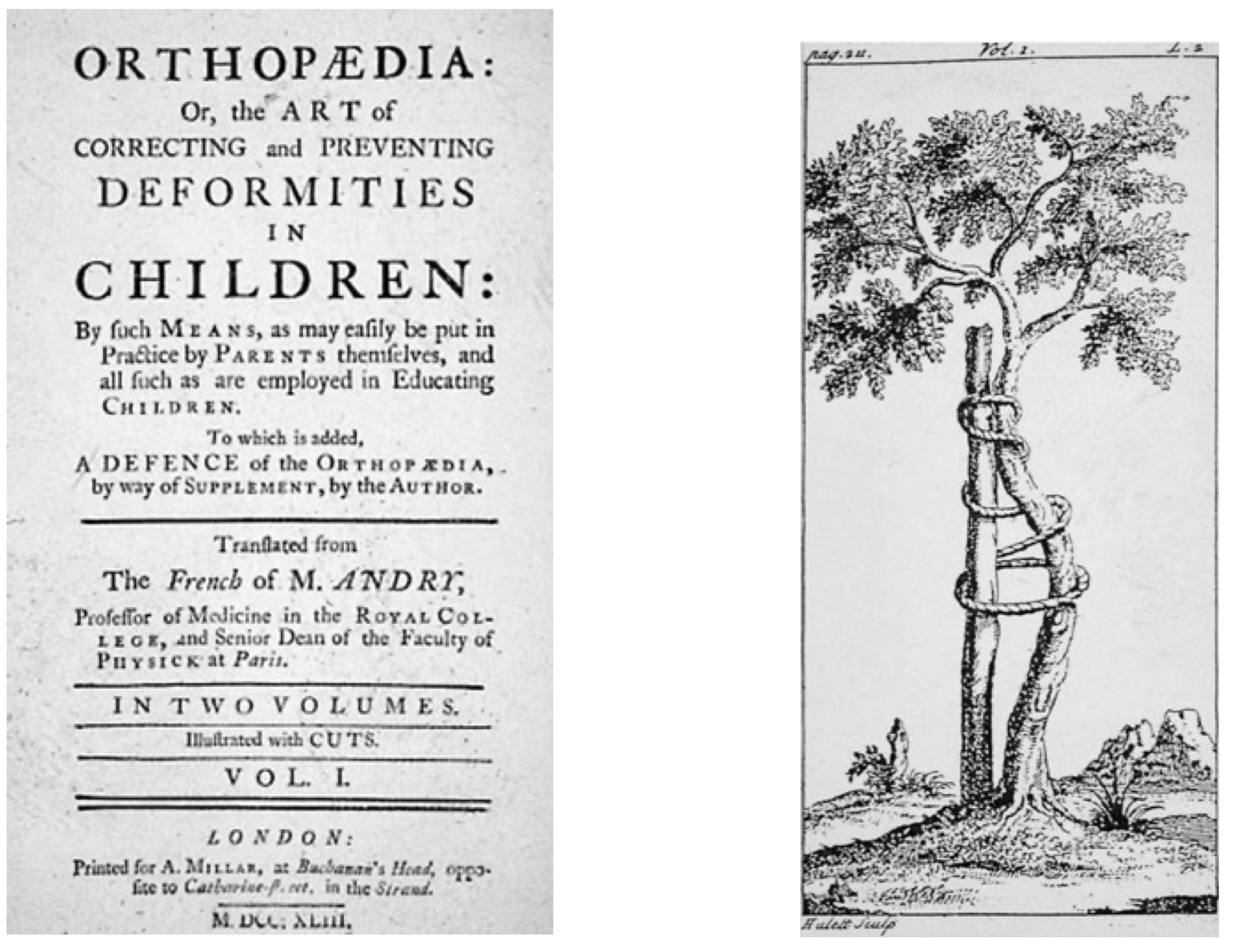
We are not proposing a perfect solution, but we are proposing honesty. It’s interesting to recall that the term “orthopaedics” was coined almost three centuries ago, with the etymology showing us its non-surgical roots—at its foundation, it was originally about enhancing proper development of children.[5]
Orthopaedics: in the beginning, it was about assisting with DEVELOPMENT and GROWTH…
Point is: The modern world of joint replacement and spinal reconstruction is not where orthopedics began. It all started with the notion of helping our kids grow up straight and healthy.
So, it’s with this in mind that we propose a name such as Pediatric- or Developmental-Dentofacial Orthopedics to better capture the scope and responsibility of the work.
What’s in a name?
This one would signal out loud that this is not merely about alignment of teeth, but foundationally also about development of adjacent functional biological real estate. This is not just about appearance, anymore. This is foundationally about function—and, as we mentioned above, function inevitably follows form.
Such a shift would not solve every controversy or erase past harms, but it would guide us past Cicero’s “softened name” problem and widen the lens through which future decisions are made, reminding practitioners, parents, and policymakers alike, that the stakes are larger than straight teeth.
That’s a thought worth smiling about—and acting on.
Kind mojo,
Kev & Dave
Kevin Boyd, DDS, MSC
Chief Dental Officer, Rebis Health
David E. McCarty, MD, FAASM
Chief Medical Officer, Rebis Health
Co-Creator (with Ellen Stothard, PhD) of the Empowered Sleep Apnea project
References
McCarty DE, Hang WM, Stothard E. Empowered Sleep Apnea: THE PODCAST. Season 2, Episode 8: THE TALE OF THREE FACES Published online 3/15/23.
Clark B, dir. Black Christmas. Vision IV (Canada); 1974.
4. Mew, M. (2014). Craniofacial dystrophy: A possible syndrome?British Dental Journal, 216(10), 555–558. https://doi.org/10.1038/sj.bdj.2014.401
5. Andry N. Orthopaedia; or, The Art of Correcting and Preventing Deformities in Children. London: A. Millar; 1743.
NB: This essay originally appeared in the mighty SLEEP REVIEW magazine, published online 26 February 2026. Please click the link and visit the essay in its native habitat…scroll to the bottom and you will see the essay is sparking some good discussion, with hopefully more to come…This special “Dave’s Notes” version of the essay includes the iconic image of the developing tree, from the first textbook on “orthopedics” — literally “right-growth of children”…we hope you enjoy it! —Dave