

An Open Letter to UnitedHealthcare
On Medical Ethics, Corporate Power, and the Human Cost of Fragmented Care
~ ~ ~ ~ ~
By David E. McCarty, MD, FAASM
Chief Medical Officer, Rebis Health; Co-Creator, Empowered Sleep Apnea project
26 May 2026
~ ~ ~ ~ ~
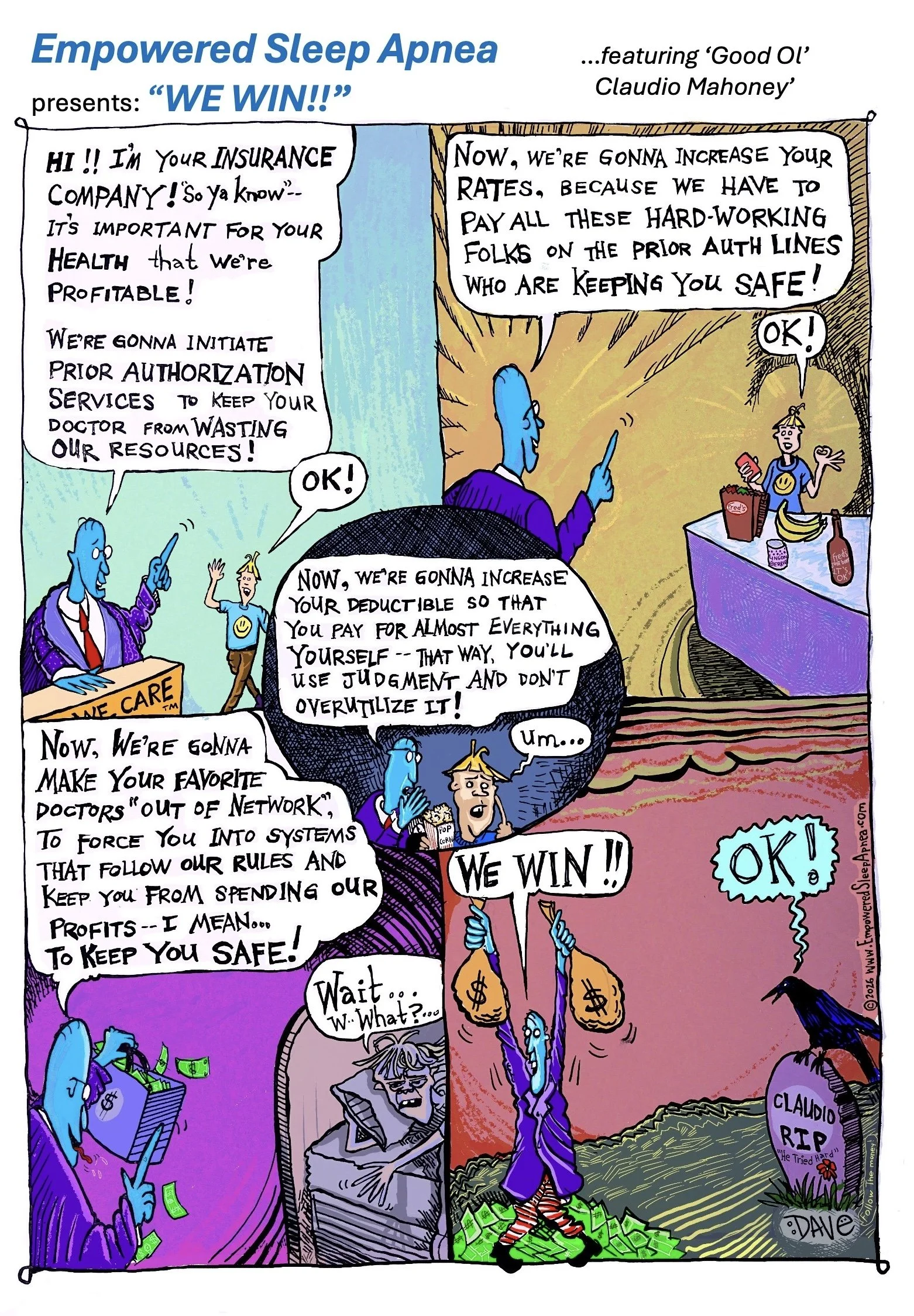
EMPOWERED SLEEP APNEA presents: “WE WIN!!”
To the leadership of UnitedHealthcare,
I am writing this publicly because private communication appears no longer possible.
Our organization in Colorado recently learned that UnitedHealthcare chose to terminate its relationship with our IPA after decades of caring for a shared patient population. Following that decision, our attempts at dialogue repeatedly went unanswered. Meanwhile, many patients were told a simple story: that our physicians demanded unreasonable compensation and forced your hand.
The fact that this narrative is FALSE will serve as a starting point, but I don’t want to get into that. The important part is that all of the finger-pointing distracts from a much larger and more foundational question:
What ethical obligations does a modern healthcare corporation owe to the human beings whose lives are altered by its decisions?
As a physician, I was trained within the framework of the Four Principles of Medical Ethics articulated by Beauchamp and Childress in Principles of Biomedical Ethics (1979): autonomy, beneficence, non-maleficence, and justice.[1–4] These principles did not emerge in a vacuum. They arose in the aftermath of medicine’s moral catastrophes: Tuskegee, Willowbrook, and other institutional failures that demonstrated how easily systems claiming to serve humanity can drift away from the humans themselves.[2,5,6]
These principles were meant to function as guardrails against inhumane and unethical care.
From where many of us stand in the field, UnitedHealthcare’s behavior in situations like this appears increasingly difficult to reconcile with these principles.
Please allow me to expound…
~ ~ ~ ~ ~
AUTONOMY
Autonomy requires honest communication and meaningful patient choice.
Yet patients were abruptly informed that longstanding physician relationships were disappearing under circumstances they did not fully understand. Narratives were supplied for them. Decisions were made far away from them. Continuity (one of the deepest forms of medical trust) became collateral damage.
The medical literature is unambiguous on this point. Continuity of care is associated with improved outcomes, fewer emergency visits, fewer hospitalizations, and even lower mortality.[7–9] Conversely, disruption of established patient-provider relationships increases emergency utilization and worsens outcomes in vulnerable populations.[7,8]
To patients, these relationships are not “network units.” They are lifelines.
~ ~ ~ ~ ~
BENEFICENCE
Beneficence asks whether systems are genuinely acting in the best interests of patients.
But when prior authorization barriers, opaque administrative decisions, and narrowing networks become normalized features of care, patients increasingly experience not stewardship, but exhaustion.
A growing body of evidence demonstrates that prior authorization delays are associated with disease exacerbation, preventable hospitalization, prolonged hospital stays, and adverse clinical outcomes across multiple specialties.[10,11] In a 2023 AMA survey, 94% of physicians reported care delays associated with prior authorization requirements, while nearly one-quarter reported serious adverse events including hospitalization, disability, and death.[11] This is not collaboration, folks. This is attrition.
~ ~ ~ ~ ~
NON-MALEFICENCE
“First, do no harm” extends beyond surgical complications and medication errors.
Harm also occurs when frightened patients lose trusted care teams.
Harm occurs when delays destabilize treatment plans.
Harm occurs when administrative systems generate confusion, fear, abandonment, and helplessness while insisting these same mechanisms exist “for patient safety.”
Increasingly, physicians themselves are being harmed as well. Administrative utilization-management burdens have become strongly associated with physician burnout, moral injury, and workforce instability.[12,13]
When physicians spend 12–14 hours per week fighting authorization battles instead of caring for patients, something foundational has gone wrong.[11,13]
~ ~ ~ ~ ~
JUSTICE
Justice requires fairness, transparency, and equitable access to care.
Yet modern healthcare increasingly feels contingent upon contractual leverage, deductible engineering, network manipulation, and administrative opacity largely invisible to the people most affected by them.
Deductibles in American healthcare have risen dramatically over the last two decades.[14,15] High-deductible health plans are associated with reduced receipt of guideline-concordant care for chronic illness and sharp reductions in healthcare utilization among lower-income patients.[15,16]
At the same time, narrowing provider networks have become increasingly common, disrupting continuity and limiting meaningful patient choice.[17,18]
Patients are repeatedly told these systems exist to protect them while simultaneously watching deductibles rise, networks narrow, prior authorizations multiply, and trusted relationships dissolve.
Eventually, folks start to notice the contradiction.
~ ~ ~ ~ ~
Here it is: this is why I drew the attached cartoon! It’s not because I enjoy conflict (I don’t!), and I’m not pretending that the problem of healthcare provision is simple (it’s not!). However, satire becomes necessary when institutional language drifts too far from lived experience, and nobody returns our emails.
See, the deepest tragedy here is not financial; it’s relational.
Medicine is not merely the management of assets and contracts; it’s a human trust network built slowly over years between patients, clinicians, families, and communities. When those bonds are severed casually (or when blame is wrongly and casually displaced onto frontline clinicians after the fact!) something sacred erodes.
I suspect most of y’all who work for UnitedHealthcare entered this business with sincere intentions. However, make no mistake, folks--systems that behave like this develop their own moral inertia, one that even good people can’t seem to stop. See, institutions drift, and bureaucracies eventually begin protecting themselves first.
I just want you to know that all of us are watching you.
The ethical literature has warned us about this tension for decades. As ethicist Mark Bloche observed in JAMA, systems that incentivize physicians to restrict access to care create a painful conflict between institutional demands and the physician’s ethical obligation to patients.[20] Other scholars have similarly warned that healthcare organizations increasingly operationalize economics while rhetorically preserving the language of compassion.[21,22]
So, this letter is not merely an accusation, though I suppose it is, effectively, that. What it is, at its foundation, is a plea for reflection. I want to see if you folks can see what’s happening! See, folks, the question facing modern healthcare is no longer merely:
“How do we manage cost?”
The question is becoming:
“What kind of moral ecosystem are we creating?”
From where many of us stand in the field, the answer is becoming harder to defend.
So, enjoy the cartoon! This one’s for you! LOL!
Before we part, though, I’ll leave you with a final thought-project, for you to answer, at your leisure:
When your profits shout “WE WIN!”, I’d like somebody on your end to start clarifying exactly what that means.
Kind mojo,
Dave
David E. McCarty, MD, FAASM
Chief Medical Officer, Rebis Health; Co-Creator, Empowered Sleep Apnea project
~ ~ ~ ~ ~
References
[1] Beauchamp TL, Childress JF. Principles of Biomedical Ethics. New York: Oxford University Press; 1979.
[2] Hull SC, Mullen JB, Kirkpatrick JN. Proposal and rationale for a cardioethics curriculum. JACC Advances. 2024;3(3):100845.
[3] Gillon R. Defending the four principles approach as a good basis for good medical practice and therefore for good medical ethics. J Med Ethics. 2015;41(1):111–116.
[4] Bernat JL. Challenges to ethics and professionalism facing the contemporary neurologist. Neurology. 2014;83(14):1285–1293.
[5] Tobin MJ. Fiftieth anniversary of uncovering the Tuskegee Syphilis Study: the story and timeless lessons. Am J Respir Crit Care Med. 2022;205(10):1145–1158.
[6] Spellecy R, Busse K. The history of human subjects research and rationale for institutional review board oversight. Nutr Clin Pract. 2021;36(3):560–567.
[7] Sabety AH, Jena AB, Barnett ML. Changes in health care use and outcomes after turnover in primary care. JAMA Intern Med. 2021;181(2):186–194.
[8] Staiger B. Disruptions to the patient-provider relationship and patient utilization and outcomes: evidence from Medicaid managed care. J Health Econ. 2022;81:102574.
[9] Engström SG, André M, Arvidsson E, et al. Personal GP-continuity improves healthcare outcomes in primary care populations: a systematic review. Br J Gen Pract. 2025.
[10] Murphy J, Beauchamp N, Sun KJ, et al. Adverse effects of health plan prior authorization on clinical effectiveness and patient outcomes: a systematic review. Am J Med. 2025.
[11] Gotlieb E, Joseph B, Blank L, Jetté N. Barriers and consequences of prior authorization for neurologic medications. JAMA Neurol. 2025.
[12] Struthers A, Chapman MA, Charles PD, et al. Utilization management and physician burnout. Am J Manag Care. 2024;30(11):561–566.
[13] Chen WC, Carpenter C, Sidiqi B, et al. Integrating prior authorization into clinical workflows for care access and practitioner experience. JAMA Netw Open. 2025;8(12):e2549093.
[14] Dickman SL, Himmelstein DU, Woolhandler S. Inequality and the health-care system in the USA. Lancet. 2017;389(10077):1431–1441.
[15] Gidwani R, Yank V, Asch SM, et al. High-deductible health plans and receipt of guideline-concordant care for adults with chronic illness. JAMA Netw Open. 2025;8(4):e258045.
[16] Rabin DL, Jetty A, Petterson S, Saqr Z, Froehlich A. Among low-income respondents with diabetes, high-deductible versus no-deductible insurance sharply reduces medical service use. Diabetes Care. 2017;40(2):239–245.
[17] Graves JA, Nshuti L, Everson J, et al. Breadth and exclusivity of hospital and physician networks in US insurance markets. JAMA Netw Open. 2020;3(12):e2029419.
[18] Gaffney A, McCormick D. The Affordable Care Act: implications for health-care equity. Lancet. 2017;389(10077):1442–1452.
[19] Wang Y, Levy JF, Mattingly TJ, et al. Prior authorization and associated delays and denials of branded medication dispensation. JAMA Health Forum. 2026.
[20] Bloche MG. Clinical loyalties and the social purposes of medicine. JAMA. 1999;281(3):268–274.
[21] Berkman ND, Wynia MK, Churchill LR. Gaps, conflicts, and consensus in the ethics statements of professional associations, medical groups, and health plans. J Med Ethics. 2004;30(4):395–401.
[22] Povar GJ, Blumen H, Daniel J, et al. Ethics in practice: managed care and the changing health care environment. Ann Intern Med. 2004;141(2):131–